

Physical activity and brain function in older adults at increased risk for Alzheimer's disease
- PMID: 24961307
- PMCID: PMC4061823
- DOI: 10.3390/brainsci3010054
Physical activity and brain function in older adults at increased risk for Alzheimer's disease
Abstract
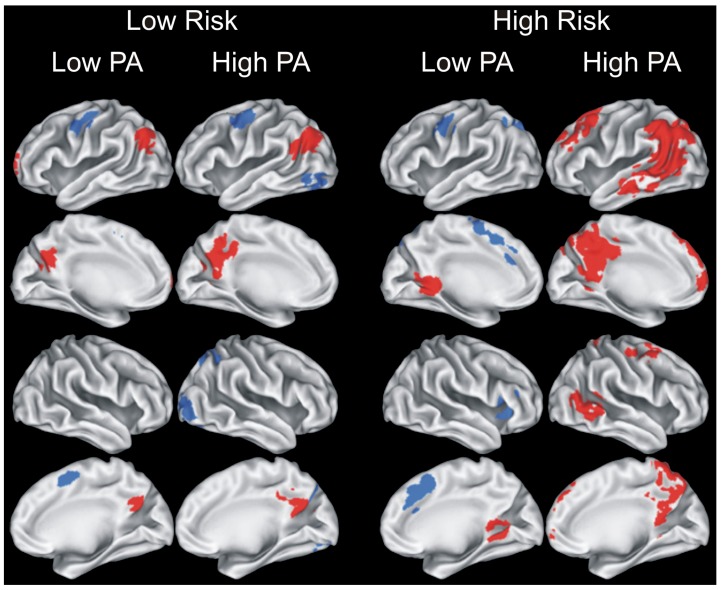
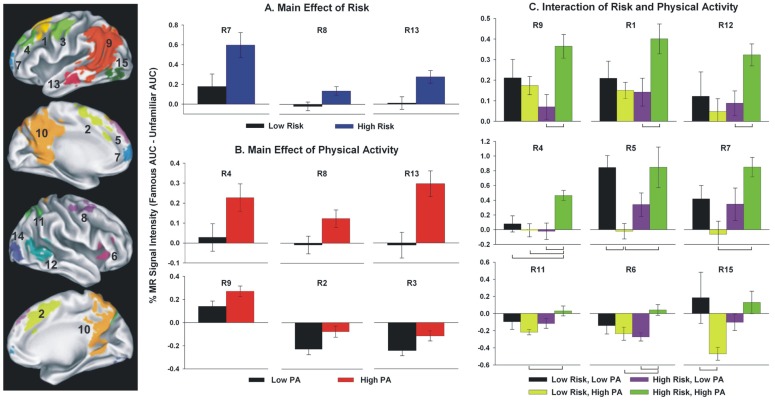
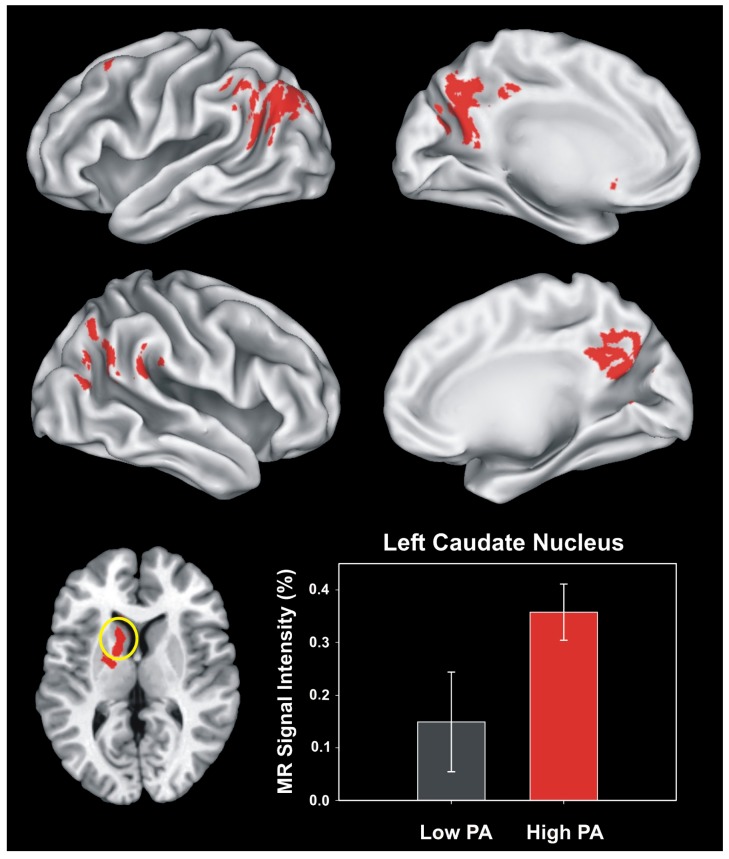
Leisure-time physical activity (PA) and exercise training are known to help maintain cognitive function in healthy older adults. However, relatively little is known about the effects of PA on cognitive function or brain function in those at increased risk for Alzheimer's disease through the presence of the apolipoproteinE epsilon4 (APOE-ε4) allele, diagnosis of mild cognitive impairment (MCI), or the presence of metabolic disease. Here, we examine the question of whether PA and exercise interventions may differentially impact cognitive trajectory, clinical outcomes, and brain structure and function among individuals at the greatest risk for AD. The literature suggests that the protective effects of PA on risk for future dementia appear to be larger in those at increased genetic risk for AD. Exercise training is also effective at helping to promote stable cognitive function in MCI patients, and greater cardiorespiratory fitness is associated with greater brain volume in early-stage AD patients. In APOE-ε4 allele carriers compared to non-carriers, greater levels of PA may be more effective in reducing amyloid burden and are associated with greater activation of semantic memory-related neural circuits. A greater research emphasis should be placed on randomized clinical trials for exercise, with clinical, behavioral, and neuroimaging outcomes in people at increased risk for AD.
Figures
Similar articles
-
Interactive effects of physical activity and APOE-ε4 on white matter tract diffusivity in healthy elders.Neuroimage. 2016 May 1;131:102-12. doi: 10.1016/j.neuroimage.2015.08.007. Epub 2015 Aug 8. Neuroimage. 2016. PMID: 26265157 Free PMC article.
-
Interactive effects of physical activity and APOE-ε4 on BOLD semantic memory activation in healthy elders.Neuroimage. 2011 Jan 1;54(1):635-44. doi: 10.1016/j.neuroimage.2010.07.070. Epub 2010 Aug 5. Neuroimage. 2011. PMID: 20691792 Free PMC article.
-
Exercise as Potential Therapeutic Target to Modulate Alzheimer's Disease Pathology in APOE ε4 Carriers: A Systematic Review.Cardiol Ther. 2021 Jun;10(1):67-88. doi: 10.1007/s40119-020-00209-z. Epub 2021 Jan 5. Cardiol Ther. 2021. PMID: 33403644 Free PMC article. Review.
-
The Effects of CSF Neurogranin and APOE ε4 on Cognition and Neuropathology in Mild Cognitive Impairment and Alzheimer's Disease.Front Aging Neurosci. 2021 Apr 27;13:667899. doi: 10.3389/fnagi.2021.667899. eCollection 2021. Front Aging Neurosci. 2021. PMID: 33986657 Free PMC article.
-
Interaction between physical exercise and APOE gene polymorphism on cognitive function in older people.Braz J Med Biol Res. 2020 Dec 9;54(2):e10098. doi: 10.1590/1414-431X202010098. eCollection 2020. Braz J Med Biol Res. 2020. PMID: 33331535 Free PMC article. Review.
Cited by
-
A systematic review and meta-analysis of the effects of physical exercise on white matter integrity and cognitive function in older adults.Geroscience. 2024 Apr;46(2):2641-2651. doi: 10.1007/s11357-023-01033-8. Epub 2023 Dec 18. Geroscience. 2024. PMID: 38108993 Free PMC article.
-
Cognitive Functioning Differences Between Physically Active and Sedentary Older Adults.J Alzheimers Dis Rep. 2018 May 26;2(1):93-101. doi: 10.3233/ADR-180053. J Alzheimers Dis Rep. 2018. PMID: 30480252 Free PMC article.
-
Exercise improves cognitive function in aging patients.Int J Clin Exp Med. 2014 Oct 15;7(10):3144-9. eCollection 2014. Int J Clin Exp Med. 2014. PMID: 25419345 Free PMC article.
-
Targeting Neuroinflammation to Treat Alzheimer's Disease.CNS Drugs. 2017 Dec;31(12):1057-1082. doi: 10.1007/s40263-017-0483-3. CNS Drugs. 2017. PMID: 29260466 Free PMC article. Review.
-
Synergistic effects of quercetin and regular exercise on the recovery of spatial memory and reduction of parameters of oxidative stress in animal model of Alzheimer's disease.EXCLI J. 2020 May 8;19:596-612. doi: 10.17179/excli2019-2082. eCollection 2020. EXCLI J. 2020. PMID: 32483406 Free PMC article.
References
-
- Yaffe K., Fox P., Newcomer R., Sands L., Lindquist K., Dane K., Covinsky K.E. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002;287:2090–2097. - PubMed
-
- Yaffe K., Petersen R.C., Lindquist K., Kramer J., Miller B. Subtype of mild cognitive impairment and progression to dementia and death. Dement. Geriatr. Cogn. Dis. 2006;22:312–319. - PubMed
-
- Alzheimer’s Association 2012 Alzheimer’s disease facts and figures. Alzheimers Dement. 2012;8:131–168. - PubMed
-
- Daviglus M.L., Bell C.C., Berrettini W., Bowen P.E., Connolly E.S., Cox N.J., Dunbar-Jacob J.M., Granieri E.C., Hunt G., McGarry K., et al. NIH State-of-the-Science Conference Statement: Preventing Alzheimer’s Disease and Cognitive Decline. NIH Consens. State Sci. Statements. 2010;27:1–30. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
