

Effect of protective ventilation on postoperative pulmonary complications in patients undergoing general anaesthesia: a meta-analysis of randomised controlled trials
- PMID: 24961718
- PMCID: PMC4078782
- DOI: 10.1136/bmjopen-2014-005208
Effect of protective ventilation on postoperative pulmonary complications in patients undergoing general anaesthesia: a meta-analysis of randomised controlled trials
Abstract
Objective: To determine whether anaesthetised patients undergoing surgery could benefit from intraoperative protective ventilation strategies.
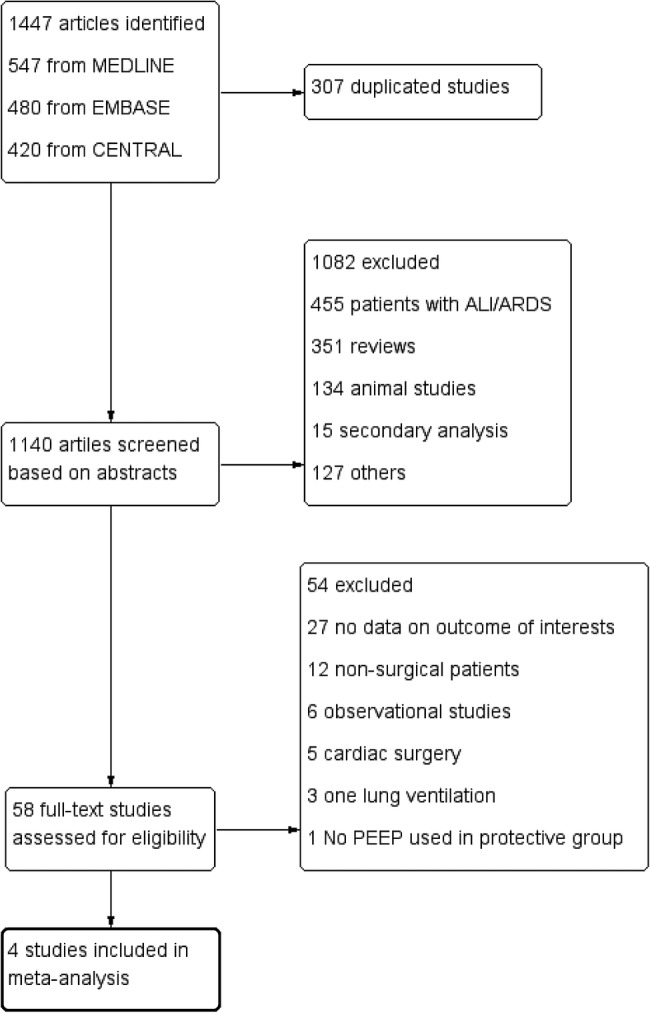
Methods: MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials (CENTRAL) were searched up to February 2014. Eligible studies evaluated protective ventilation versus conventional ventilation in anaesthetised patients without lung injury at the onset of mechanical ventilation. The primary outcome was the incidence of postoperative pulmonary complications. Included studies must report at least one of the following end points: the incidence of atelectasis or acute lung injury or pulmonary infections.
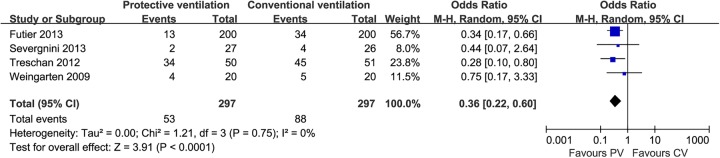
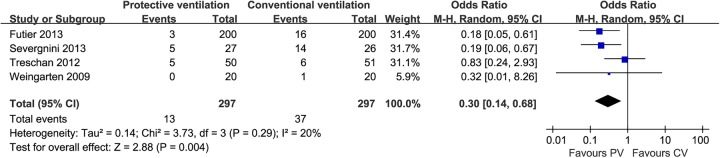
Results: Four studies (594 patients) were included. Meta-analysis using a random effects model showed a significant decrease in the incidence of atelectasis (OR=0.36; 95% CI 0.22 to 0.60; p<0.0001; I(2)=0%) and pulmonary infections (OR=0.30; 95% CI 0.14 to 0.68; p=0.004; I(2)=20%) in patients receiving protective ventilation. Ventilation with protective strategies did not reduce the incidence of acute lung injury (OR=0.40; 95% CI 0.07 to 2.15; p=0.28; I(2)=12%), all-cause mortality (OR=0.77; 95% CI 0.33 to 1.79; p=0.54; I(2)=0%), length of hospital stay (weighted mean difference (WMD)=-0.52 day, 95% CI -4.53 to 3.48 day; p=0.80; I(2)=63%) or length of intensive care unit stay (WMD=-0.55 day, 95% CI -2.19 to 1.09 day; p=0.51; I(2)=39%).
Conclusions: Intraoperative use of protective ventilation strategies has the potential to reduce the incidence of postoperative pulmonary complications in patients undergoing general anaesthesia. Prospective, well-designed clinical trials are warranted to confirm the beneficial effects of protective ventilation strategies in surgical patients.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

References
-
- Arozullah AM, Khuri SF, Henderson WG, et al. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med 2001;135:847–57 - PubMed
-
- Hedenstierna G, Edmark L. The effects of anesthesia and muscle paralysis on the respiratory system. Intensive Care Med 2005;31:1327–35 - PubMed
-
- Shander A, Fleisher LA, Barie PS, et al. Clinical and economic burden of postoperative pulmonary complications: patient safety summit on definition, risk-reducing interventions, and preventive strategies. Crit Care Med 2011;39:2163–72 - PubMed
-
- Lawrence VA, Cornell JE, Smetana GW. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006;144:596–608 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical