

The economic burden of pediatric gastroenteritis to Bolivian families: a cross-sectional study of correlates of catastrophic cost and overall cost burden
- PMID: 24962128
- PMCID: PMC4094680
- DOI: 10.1186/1471-2458-14-642
The economic burden of pediatric gastroenteritis to Bolivian families: a cross-sectional study of correlates of catastrophic cost and overall cost burden
Abstract
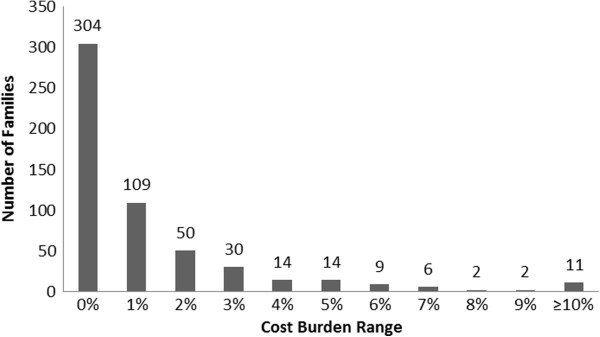
Background: Worldwide, acute gastroenteritis causes substantial morbidity and mortality in children less than five years of age. In Bolivia, which has one of the lower GDPs in South America, 16% of child deaths can be attributed to diarrhea, and the costs associated with diarrhea can weigh heavily on patient families. To address this need, the study goal was to identify predictors of cost burden (diarrhea-related costs incurred as a percentage of annual income) and catastrophic cost (cost burden ≥ 1% of annual household income).
Methods: From 2007 to 2009, researchers interviewed caregivers (n = 1,107) of pediatric patients (<5 years old) seeking treatment for diarrhea in six Bolivian hospitals. Caregivers were surveyed on demographics, clinical symptoms, direct (e.g. medication, consult fees), and indirect (e.g. lost wages) costs. Multivariate regression models (n = 551) were used to assess relationships of covariates to the outcomes of cost burden (linear model) and catastrophic cost (logistic model).
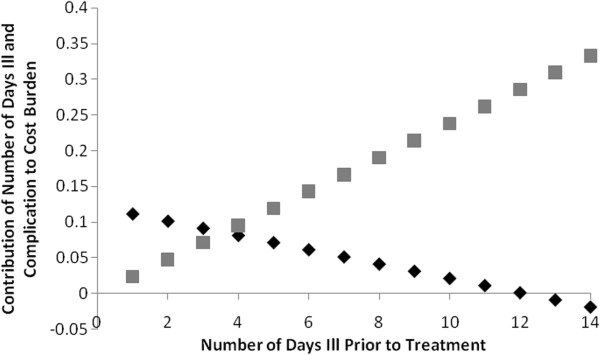
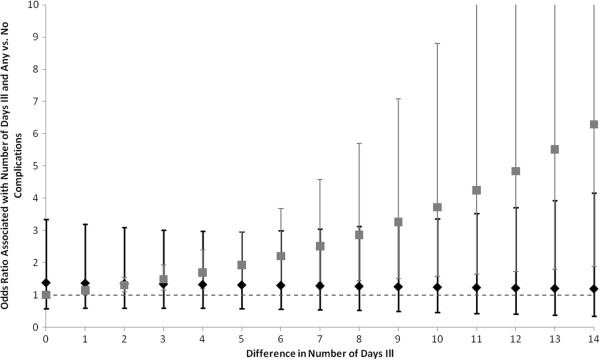
Results: We determined that cost burden and catastrophic cost shared the same significant (p < 0.05) predictors. In the logistic model that also controlled for child sex, child age, household size, rural residence, transportations taken to the current visit, whether the child presented with complications, and whether this was the child's first episode of diarrhea, significant predictors of catastrophic cost included outpatient status (OR 0.16, 95% CI [0.07, 0.37]); seeking care at a private hospital (OR 4.12, 95% CI [2.30, 7.41]); having previously sought treatment for this diarrheal episode (OR 3.92, 95% CI [1.64, 9.35]); and the number of days the child had diarrhea prior to the current visit (OR 1.14, 95% CI [1.05, 1.24]).
Conclusions: Our analysis highlights the economic impact of pediatric diarrhea from the familial perspective and provides insight into potential areas of intervention to reduce associated economic burden.
Figures
References
-
- Ehrenkranz P, Lanata CF, Penny ME, Salazar-Lindo E, Glass RI. Rotavirus diarrhea disease burden in Peru: the need for a rotavirus vaccine and its potential cost savings. Pan Am J Public Health. 2001;10(4):240–248. - PubMed
-
- Fischer TK, Anh DD, Antil L, Cat NDL, Kilgore PE, Thiem VD, Rheingans R, Tho LH, Glass RI, Bresee JS. Health care costs of diarrheal disease and estimates of the cost-effectiveness of rotavirus vaccination in Vietnam. J Infect Dis. 2005;192:1720–1726. - PubMed
-
- Podewils LJ, Antil L, Hummelman E, Bresee J, Parashar UD, Rheingans R. Projected cost-effectiveness of rotavirus vaccination for children in Asia. J Infect Dis. 2005;192:S133–S145. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
