

Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis
- PMID: 24963568
- PMCID: PMC4127879
- DOI: 10.1056/NEJMoa1312884
Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis
Abstract
Background: Cryptococcal meningitis accounts for 20 to 25% of acquired immunodeficiency syndrome-related deaths in Africa. Antiretroviral therapy (ART) is essential for survival; however, the question of when ART should be initiated after diagnosis of cryptococcal meningitis remains unanswered.
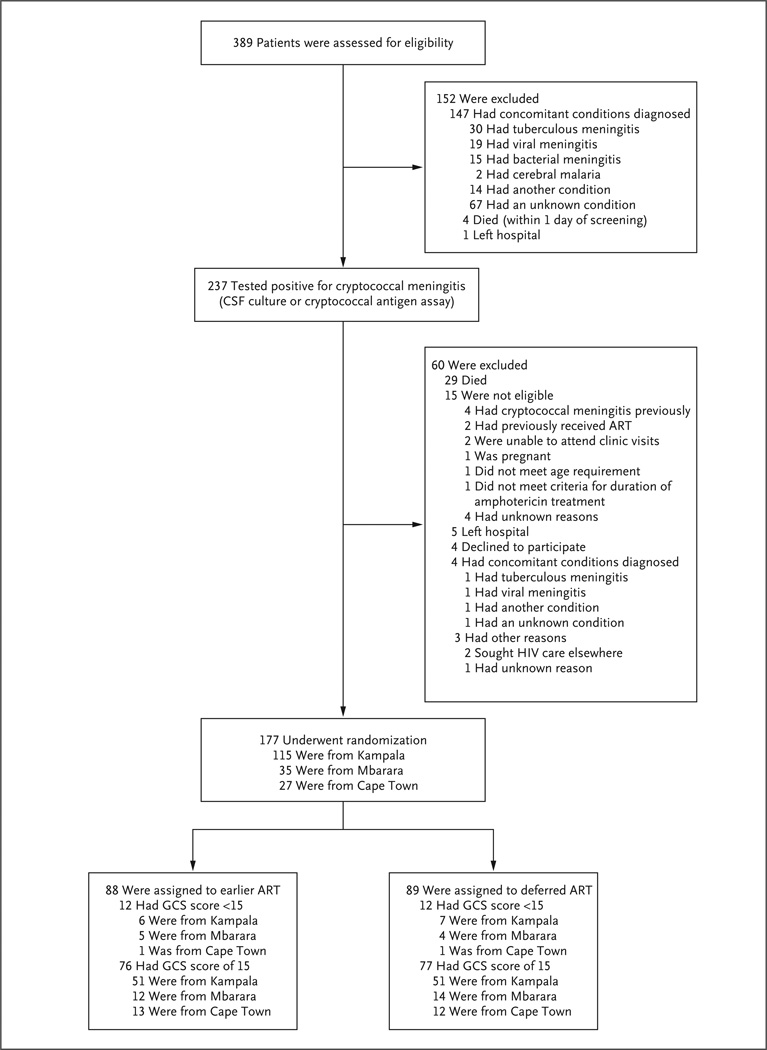
Methods: We assessed survival at 26 weeks among 177 human immunodeficiency virus-infected adults in Uganda and South Africa who had cryptococcal meningitis and had not previously received ART. We randomly assigned study participants to undergo either earlier ART initiation (1 to 2 weeks after diagnosis) or deferred ART initiation (5 weeks after diagnosis). Participants received amphotericin B (0.7 to 1.0 mg per kilogram of body weight per day) and fluconazole (800 mg per day) for 14 days, followed by consolidation therapy with fluconazole.
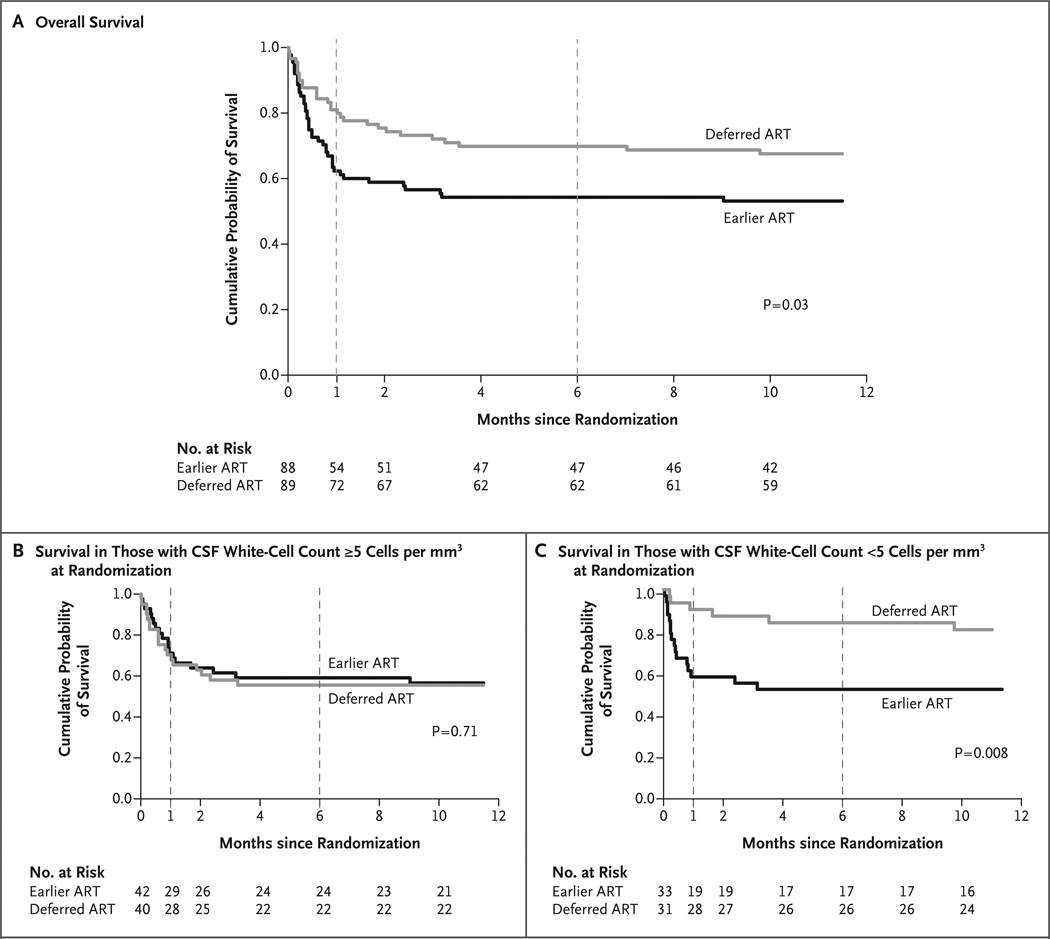
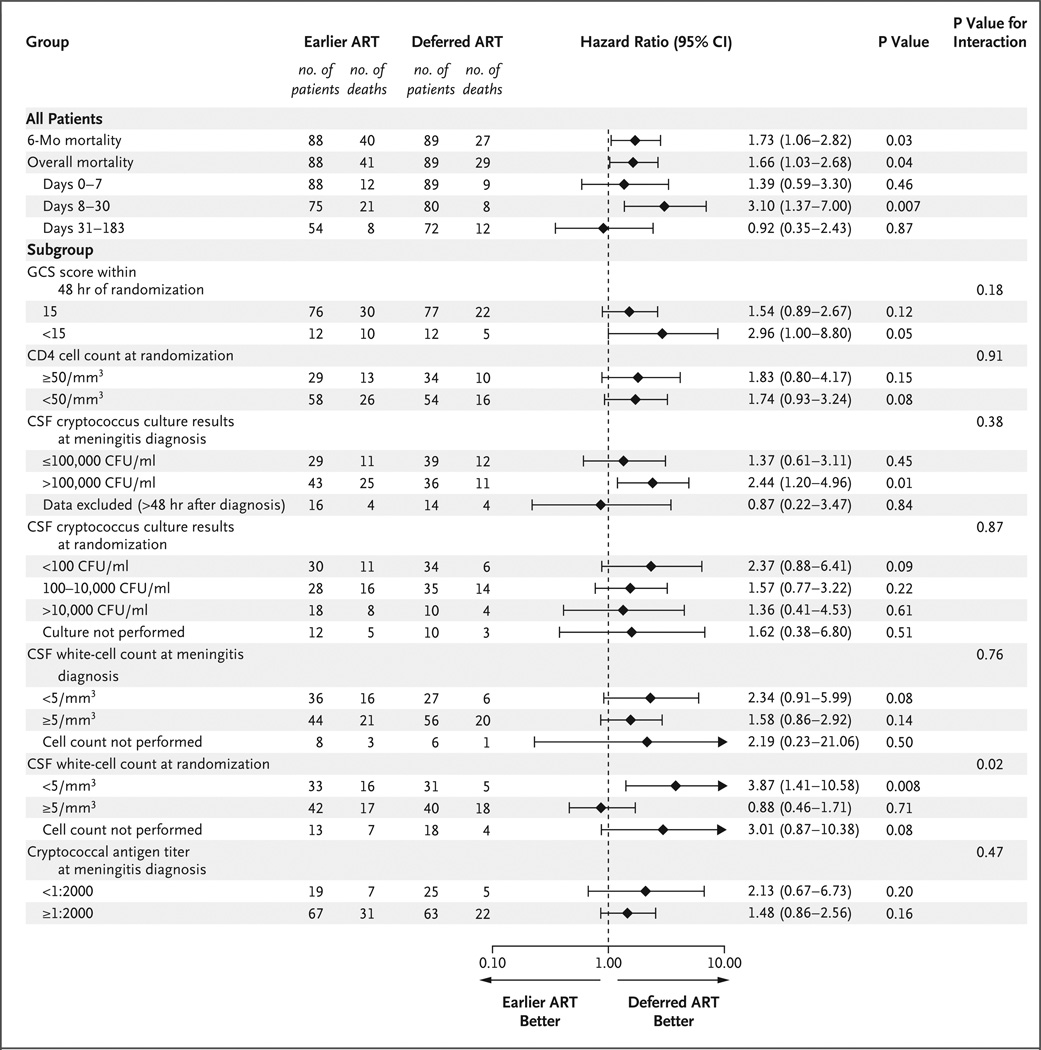
Results: The 26-week mortality with earlier ART initiation was significantly higher than with deferred ART initiation (45% [40 of 88 patients] vs. 30% [27 of 89 patients]; hazard ratio for death, 1.73; 95% confidence interval [CI], 1.06 to 2.82; P=0.03). The excess deaths associated with earlier ART initiation occurred 2 to 5 weeks after diagnosis (P=0.007 for the comparison between groups); mortality was similar in the two groups thereafter. Among patients with few white cells in their cerebrospinal fluid (<5 per cubic millimeter) at randomization, mortality was particularly elevated with earlier ART as compared with deferred ART (hazard ratio, 3.87; 95% CI, 1.41 to 10.58; P=0.008). The incidence of recognized cryptococcal immune reconstitution inflammatory syndrome did not differ significantly between the earlier-ART group and the deferred-ART group (20% and 13%, respectively; P=0.32). All other clinical, immunologic, virologic, and microbiologic outcomes, as well as adverse events, were similar between the groups.
Conclusions: Deferring ART for 5 weeks after the diagnosis of cryptococcal meningitis was associated with significantly improved survival, as compared with initiating ART at 1 to 2 weeks, especially among patients with a paucity of white cells in cerebrospinal fluid. (Funded by the National Institute of Allergy and Infectious Diseases and others; COAT ClinicalTrials.gov number, NCT01075152.).
Figures
Comment in
-
Reducing central nervous system complications associated with the human immunodeficiency virus.J Neurol. 2014 Sep;261(9):1842-5. doi: 10.1007/s00415-014-7466-9. J Neurol. 2014. PMID: 25119844 No abstract available.
-
Antiretroviral therapy after cryptococcal meningitis.N Engl J Med. 2014 Sep 18;371(12):1166-7. doi: 10.1056/NEJMc1409052. N Engl J Med. 2014. PMID: 25229929 No abstract available.
-
Antiretroviral therapy after cryptococcal meningitis.N Engl J Med. 2014 Sep 18;371(12):1165. doi: 10.1056/NEJMc1409052. N Engl J Med. 2014. PMID: 25229930 No abstract available.
-
Antiretroviral therapy after cryptococcal meningitis.N Engl J Med. 2014 Sep 18;371(12):1166. doi: 10.1056/NEJMc1409052. N Engl J Med. 2014. PMID: 25229931 No abstract available.
-
Delaying initiation of ART for 5 weeks improves survival in patients with HIV infection with cyrptococcal meningitis.Evid Based Med. 2015 Feb;20(1):15. doi: 10.1136/ebmed-2014-110073. Epub 2014 Oct 30. Evid Based Med. 2015. PMID: 25358332 No abstract available.
References
-
- Cohen DB, Zijlstra EE, Mukaka M, et al. Diagnosis of cryptococcal and tuberculous meningitis in a resource-limited African setting. Trop Med Int Health. 2010;15:910–917. - PubMed
-
- Group for Enteric, Respiratory and Meningeal Disease Surveillance in South Africa. GERMS-SA annual report. Johannesburg: National Institute for Communicable Diseases; http://www.nicd.ac.za/assets/files/GERMS-SA%202012%20Annual %20Report.pdf)
-
- Hakim JG, Gangaidzo IT, Heyderman RS, et al. Impact of HIV infection on meningitis in Harare, Zimbabwe: a prospective study of 406 predominantly adult patients. AIDS. 2000;14:1401–1407. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- K23AI073192/AI/NIAID NIH HHS/United States
- K24AI096925/AI/NIAID NIH HHS/United States
- U01AI089244/AI/NIAID NIH HHS/United States
- T32 AI055433/AI/NIAID NIH HHS/United States
- K23 AI073192/AI/NIAID NIH HHS/United States
- T32AI055433/AI/NIAID NIH HHS/United States
- U01 AI089244/AI/NIAID NIH HHS/United States
- D43 TW009771/TW/FIC NIH HHS/United States
- R34 AI081554/AI/NIAID NIH HHS/United States
- K24 AI096925/AI/NIAID NIH HHS/United States
- 081667/WT_/Wellcome Trust/United Kingdom
- 098316/WT_/Wellcome Trust/United Kingdom
- 087540/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical