

COX-2 inhibition potentiates antiangiogenic cancer therapy and prevents metastasis in preclinical models
- PMID: 24964992
- PMCID: PMC6309995
- DOI: 10.1126/scitranslmed.3008455
COX-2 inhibition potentiates antiangiogenic cancer therapy and prevents metastasis in preclinical models
Abstract
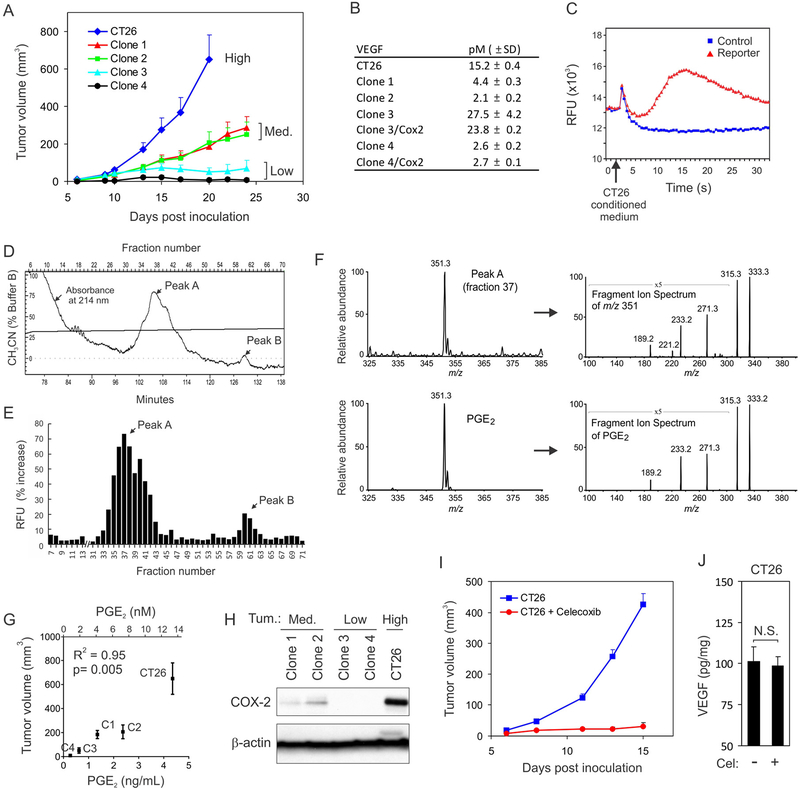
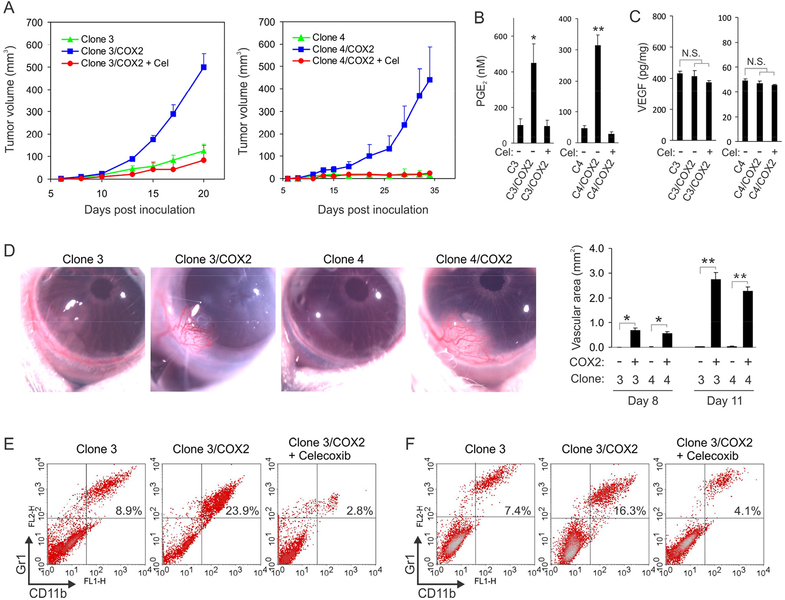
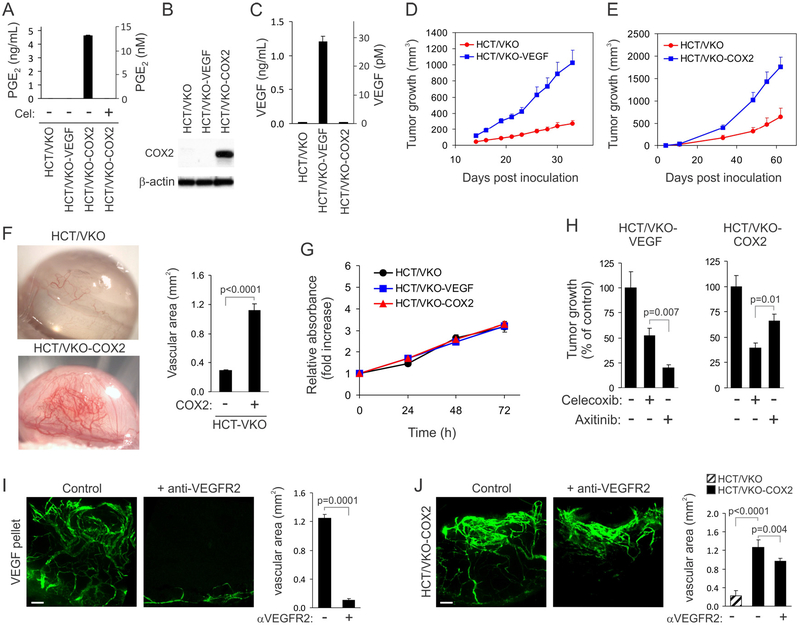
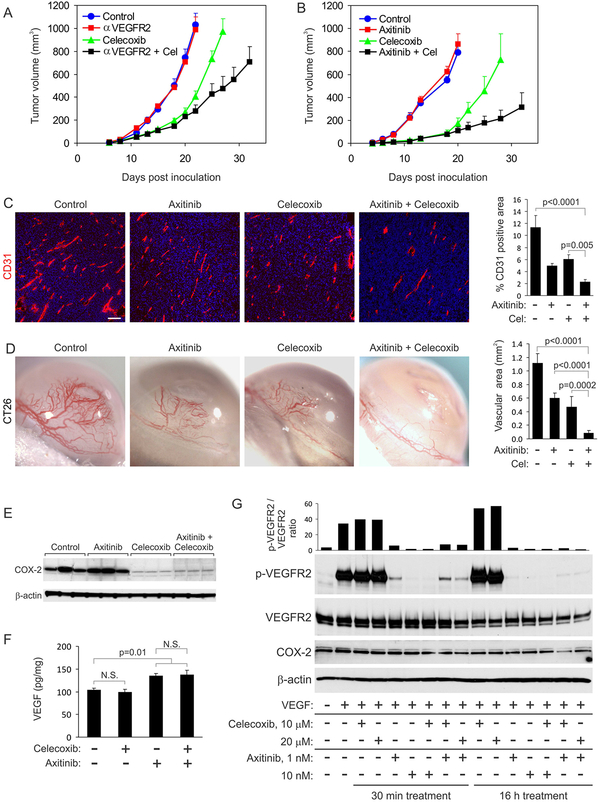
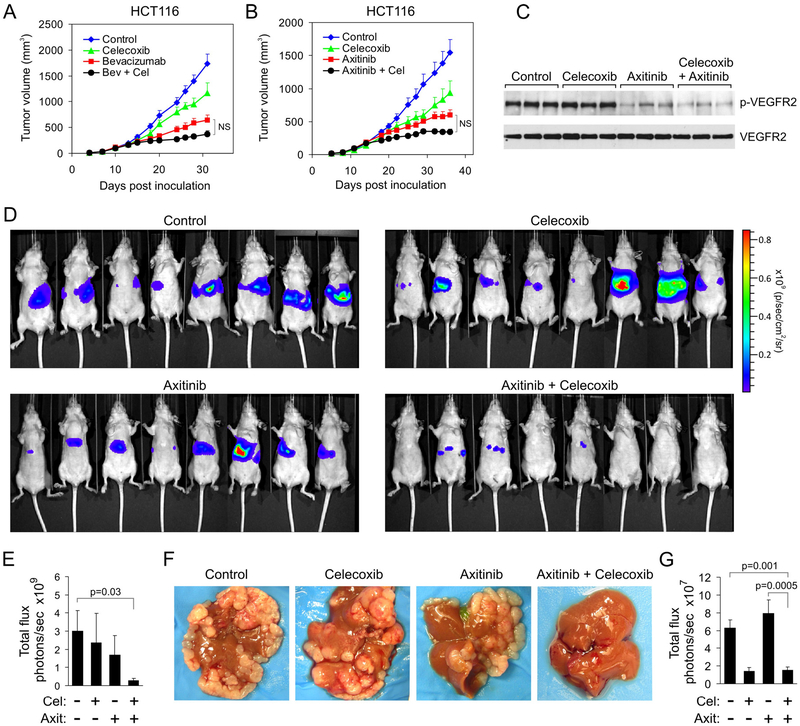
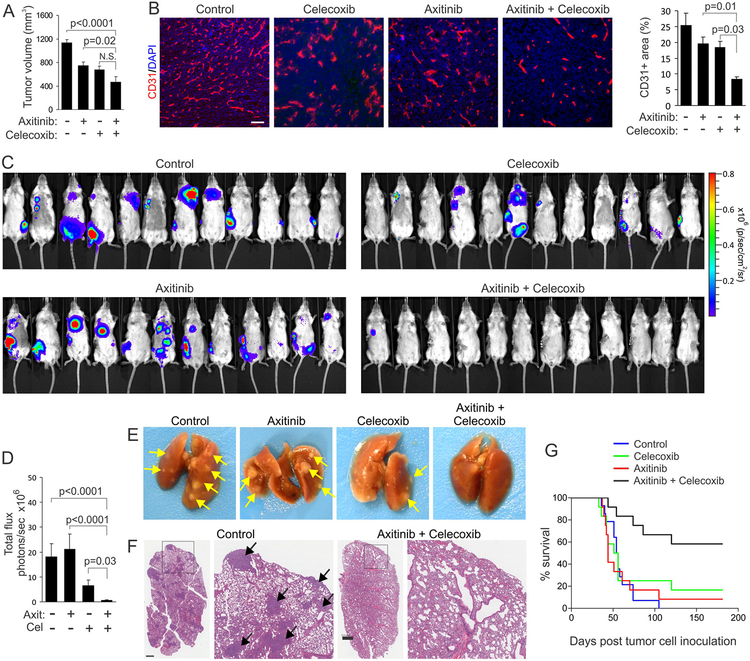
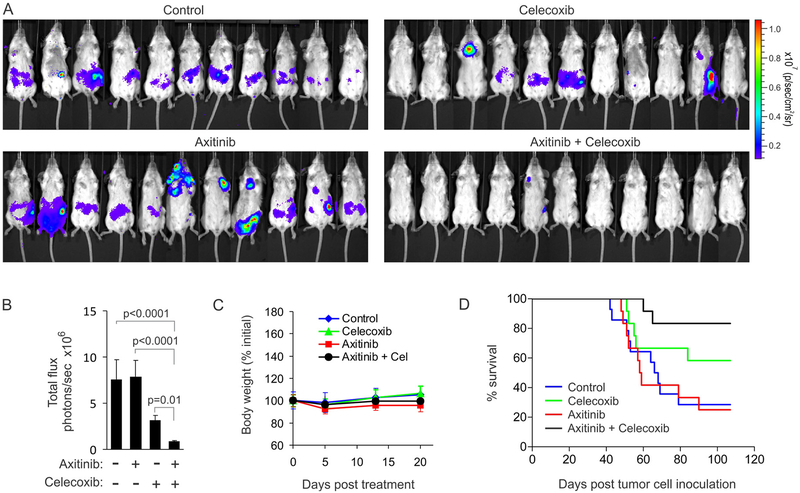
Antiangiogenic agents that block vascular endothelial growth factor (VEGF) signaling are important components of current cancer treatment modalities but are limited by alternative ill-defined angiogenesis mechanisms that allow persistent tumor vascularization in the face of continued VEGF pathway blockade. We identified prostaglandin E2 (PGE2) as a soluble tumor-derived angiogenic factor associated with VEGF-independent angiogenesis. PGE2 production in preclinical breast and colon cancer models was tightly controlled by cyclooxygenase-2 (COX-2) expression, and COX-2 inhibition augmented VEGF pathway blockade to suppress angiogenesis and tumor growth, prevent metastasis, and increase overall survival. These results demonstrate the importance of the COX-2/PGE2 pathway in mediating resistance to VEGF pathway blockade and could aid in the rapid development of more efficacious anticancer therapies.
Copyright © 2014, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
Chemoprevention of metastasis.Oncotarget. 2014 Aug 30;5(16):6556-7. doi: 10.18632/oncotarget.2382. Oncotarget. 2014. PMID: 25179303 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
