

Impact of early daycare on healthcare resource use related to upper respiratory tract infections during childhood: prospective WHISTLER cohort study
- PMID: 24965189
- PMCID: PMC4098954
- DOI: 10.1186/1741-7015-12-107
Impact of early daycare on healthcare resource use related to upper respiratory tract infections during childhood: prospective WHISTLER cohort study
Abstract
Background: Daycare attendance is an established risk factor for upper respiratory tract infections (URTI) and acute otitis media (AOM). Whether this results in higher use of healthcare resources during childhood remains unknown. We aim to assess the effect of first year daycare attendance on the timing and use of healthcare resources for URTI and AOM episodes during early childhood.
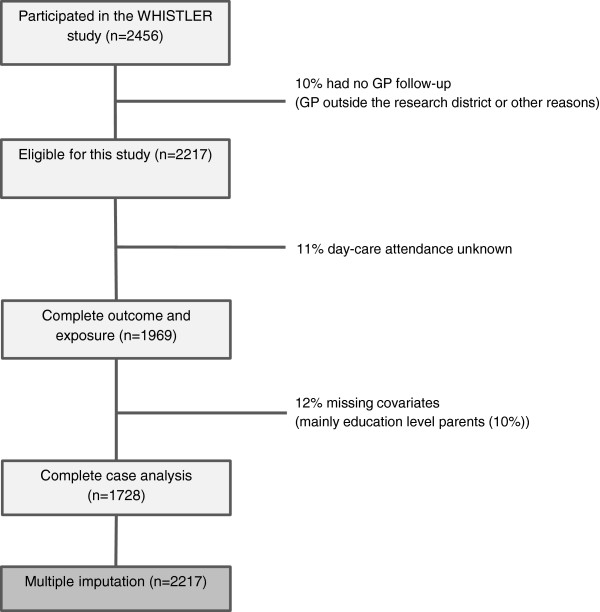
Methods: In the Wheezing-Illnesses-STudy-LEidsche-Rijn birth cohort, 2,217 children were prospectively followed up to age six years. Children were categorized according to first-year daycare attendance (yes versus no) and age at entry when applicable (age 0 to 2 months, 3 to 5 months and 6 to 12 months). Information on general practitioner (GP) diagnosed URTI and AOM, GP consultations, antibiotic prescriptions and specialist referral was collected from medical records. Daycare attendance was recorded by monthly questionnaires during the first year of life.
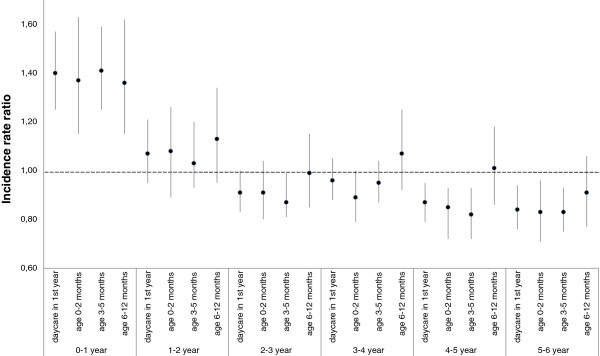
Results: First-year daycare attendees and non-attendees had similar total six-year rates of GP-diagnosed URTI and AOM episodes (59/100 child-years, 95% confidence interval 57 to 61 versus 56/100 child-years, 53 to 59). Daycare attendees had more GP-diagnosed URTI and AOM episodes before the age of one year and fewer beyond the age of four years than non-attendees (Pinteraction <0.001). Daycare attendees had higher total six-year rates for GP consultation (adjusted rate ratio 1.15, 1.00 to 1.31) and higher risk for specialist referrals (hazard ratio: 1.43, 1.01 to 2.03). The number of antibiotic prescriptions in the first six years of life was only significantly increased among children who entered daycare between six to twelve months of age (rate ratio 1.32, 1.04 to 1.67). This subgroup of child-care attendees also had the highest overall URTI and AOM incidence rates, GP consultation rates and risk for specialist referral.
Conclusions: Children who enter daycare in the first year of life, have URTI and AOM at an earlier age, leading to higher use of healthcare resources compared to non-attendees, especially when entering daycare between six to twelve months. These findings emphasize the need for improved prevention strategies in daycare facilities to lower infection rates at the early ages.
Figures
References
-
- Hak E, Rovers MM, Kuyvenhoven MM, Schellevis FG, Verheij TJ. Incidence of GP-diagnosed respiratory tract infections according to age, gender and high-risk co-morbidity: the Second Dutch National Survey of General Practice. Fam Pract. 2006;23:291–294. - PubMed
-
- Van Deursen AM, Verheij TJ, Rovers MM, Veenhoven RH, Groenwold RH, Bonten MJ, Sanders EA. Trends in primary-care consultations, comorbidities, and antibiotic prescriptions for respiratory infections in The Netherlands before implementation of pneumococcal vaccines for infants. Epidemiol Infect. 2012;140:823–834. - PubMed
-
- Brouwer CN, Rovers MM, Maille AR, Veenhoven RH, Grobbee DE, Sanders EA, Schilder AG. The impact of recurrent acute otitis media on the quality of life of children and their caregivers. Clin Otolaryngol. 2005;30:258–265. - PubMed
-
- Rovers MM. The burden of otitis media. Vaccine. 2008;26:G2–G4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
