

Long-term antiretroviral treatment initiated at primary HIV-1 infection affects the size, composition, and decay kinetics of the reservoir of HIV-1-infected CD4 T cells
- PMID: 24965451
- PMCID: PMC4136362
- DOI: 10.1128/JVI.01046-14
Long-term antiretroviral treatment initiated at primary HIV-1 infection affects the size, composition, and decay kinetics of the reservoir of HIV-1-infected CD4 T cells
Abstract
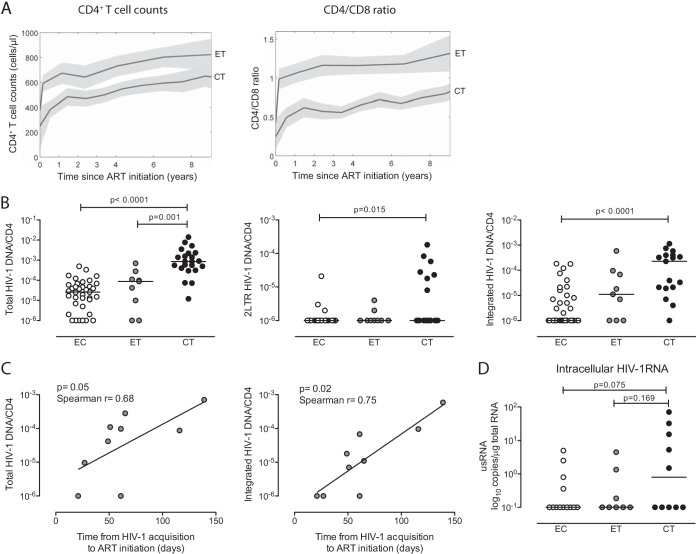
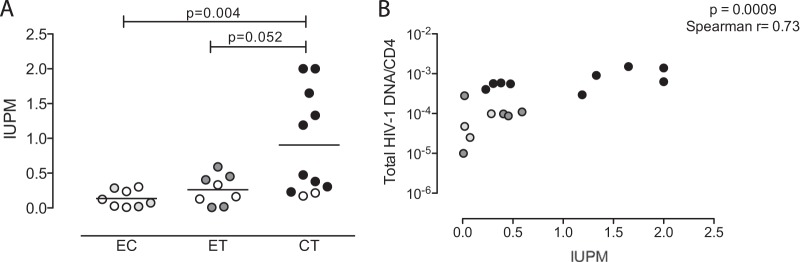
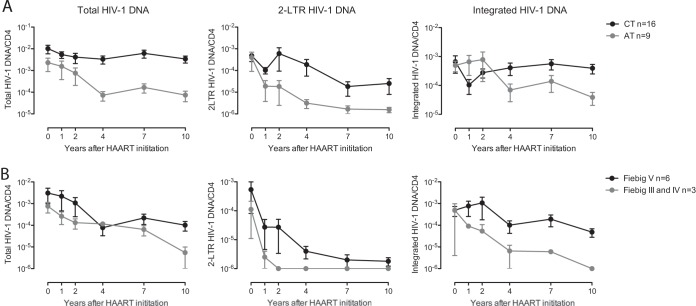
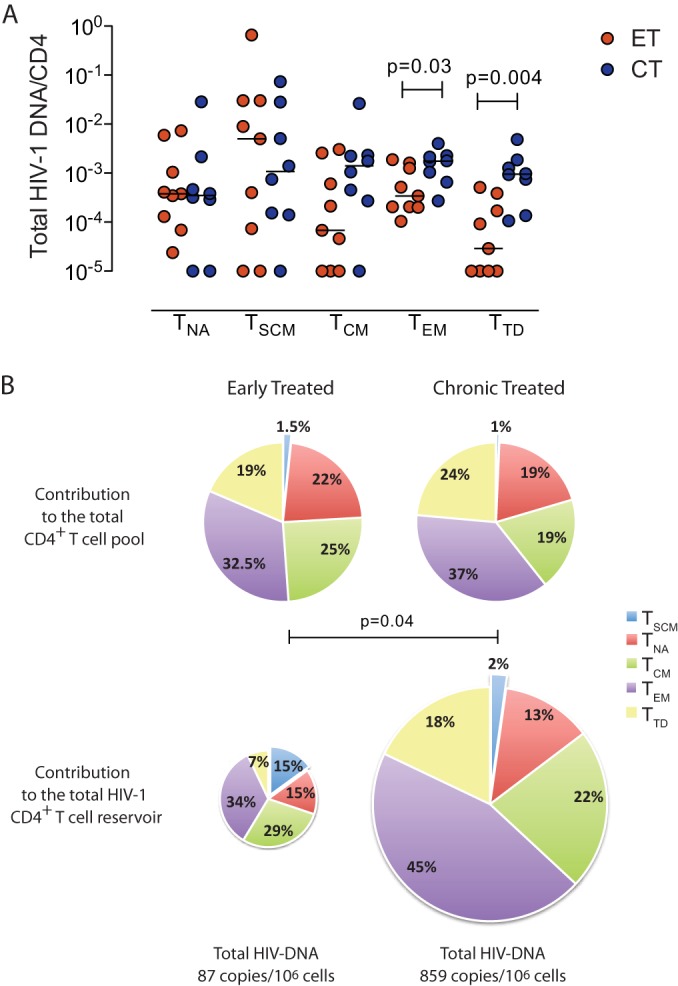
Initiation of antiretroviral therapy during the earliest stages of HIV-1 infection may limit the seeding of a long-lasting viral reservoir, but long-term effects of early antiretroviral treatment initiation remain unknown. Here, we analyzed immunological and virological characteristics of nine patients who started antiretroviral therapy at primary HIV-1 infection and remained on suppressive treatment for >10 years; patients with similar treatment duration but initiation of suppressive therapy during chronic HIV-1 infection served as controls. We observed that independently of the timing of treatment initiation, HIV-1 DNA in CD4 T cells decayed primarily during the initial 3 to 4 years of treatment. However, in patients who started antiretroviral therapy in early infection, this decay occurred faster and was more pronounced, leading to substantially lower levels of cell-associated HIV-1 DNA after long-term treatment. Despite this smaller size, the viral CD4 T cell reservoir in persons with early treatment initiation consisted more dominantly of the long-lasting central-memory and T memory stem cells. HIV-1-specific T cell responses remained continuously detectable during antiretroviral therapy, independently of the timing of treatment initiation. Together, these data suggest that early HIV-1 treatment initiation, even when continued for >10 years, is unlikely to lead to viral eradication, but the presence of low viral reservoirs and durable HIV-1 T cell responses may make such patients good candidates for future interventional studies aiming at HIV-1 eradication and cure.
Importance: Antiretroviral therapy can effectively suppress HIV-1 replication to undetectable levels; however, HIV-1 can persist despite treatment, and viral replication rapidly rebounds when treatment is discontinued. This is mainly due to the presence of latently infected CD4 T cells, which are not susceptible to antiretroviral drugs. Starting treatment in the earliest stages of HIV-1 infection can limit the number of these latently infected cells, raising the possibility that these viral reservoirs are naturally eliminated if suppressive antiretroviral treatment is continued for extremely long periods of time. Here, we analyzed nine patients who started on antiretroviral therapy within the earliest weeks of the disease and continued treatment for more than 10 years. Our data show that early treatment accelerated the decay of infected CD4 T cells and led to very low residual levels of detectable HIV-1 after long-term therapy, levels that were otherwise detectable in patients who are able to maintain a spontaneous, drug-free control of HIV-1 replication. Thus, long-term antiretroviral treatment started during early infection cannot eliminate HIV-1, but the reduced reservoirs of HIV-1 infected cells in such patients may increase their chances to respond to clinical interventions aiming at inducing a drug-free remission of HIV-1 infection.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Hecht FM, Wang L, Collier A, Little S, Markowitz M, Margolick J, Kilby JM, Daar E, Conway B, Holte S. 2006. A multicenter observational study of the potential benefits of initiating combination antiretroviral therapy during acute HIV infection. J. Infect. Dis. 194:725–733. 10.1086/506616 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K08 AI100699/AI/NIAID NIH HHS/United States
- R21 AI106468/AI/NIAID NIH HHS/United States
- R01 AI078799/AI/NIAID NIH HHS/United States
- AI106468/AI/NIAID NIH HHS/United States
- AI100699/AI/NIAID NIH HHS/United States
- R01 AI098487/AI/NIAID NIH HHS/United States
- AI089339/AI/NIAID NIH HHS/United States
- AI098487/AI/NIAID NIH HHS/United States
- 5P30AI060354-10/AI/NIAID NIH HHS/United States
- AI074415/AI/NIAID NIH HHS/United States
- AI078799/AI/NIAID NIH HHS/United States
- AI098484/AI/NIAID NIH HHS/United States
- R01 AI089339/AI/NIAID NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
- P01 AI074415/AI/NIAID NIH HHS/United States
- R56 AI098484/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
