

Review
doi: 10.1002/art.38756.
Review: unraveling Lyme disease
Affiliations
- PMID: 24965960
- PMCID: PMC4282157
- DOI: 10.1002/art.38756
Item in Clipboard
Review
Review: unraveling Lyme disease
Arthritis Rheumatol.
2014 Sep.
No abstract available
Figures
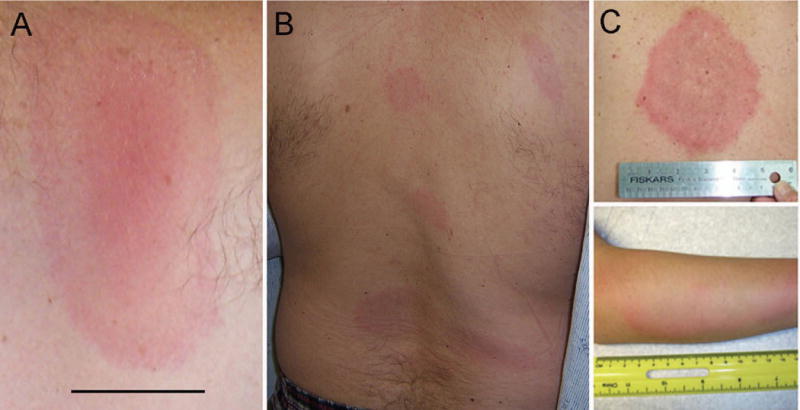
A and B, Erythema migrans presenting as a single lesion (A) (bar = 2 cm) and as multiple lesions (B). C, Skin lesion in southern tick–associated rash illness, with an appearance similar to that of erythema migrans. (Reproduced from http://www.cdc.gov/stari/symptoms/ .)
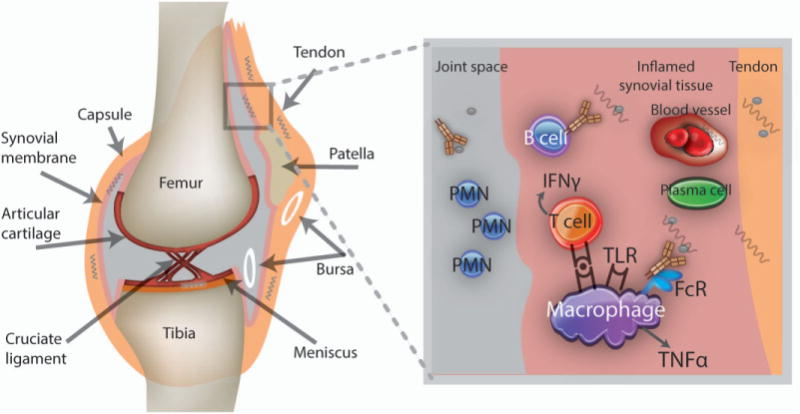
Proposed model for the initiation of Lyme arthritis. Lyme borrelia introduced into the skin disseminate hematogenously and establish infection in the joint. Borrelia in highly vascular areas such as the synovium may host-adapt to elude immune recognition by synovial immune cells and specific antibodies; others may be partially protected against these defenses because of their location in tendons, ligaments, and arteriolar walls. Months later, microdamage may expose Lyme borrelia in these latter sites or synovial resident spirochetes may be altered to suddenly become “visible,” initiating acute inflammation through Toll-like receptors (TLRs) and immune complex formation. Borrelia-specific T and B cells home to the synovium, where they contribute to the inflammatory response; lymphoid follicles may form, and with protracted inflammation, fibrinous exudates appear. These exudates may sequester Lyme borrelia and their remnants, which could also trigger inflammation if later released. In some people, the inflammatory response may become dysregulated, leading to antibiotic-refractory Lyme arthritis. Autoimmunity triggered by infection may be perpetuated when normal mechanisms of immune regulation, such as those mediated by CD25+ Treg cells, γ/δ T cells, or natural killer T cells, are deficient. Arthritis resolution occurs once residual borrelia remnants are contained and the immune response is regulated. PMN = polymorphonuclear leukocyte; IFNγ = interferon- γ; FcR = Fc receptor; TNFα = tumor necrosis factor α.
References
-
- Kurtenbach K, Hanincova K, Tsao JI, Margos G, Fish D, Ogden NH. Fundamental processes in the evolutionary ecology of Lyme borreliosis. Nat Rev Microbiol. 2006;4(9):660–9. - PubMed
-
- Steere AC, Malawista SE, Snydman DR, Shope RE, Andiman WA, Ross MR, et al. Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three connecticut communities. Arthritis Rheum. 1977;20(1):7–17. - PubMed
-
- Bockenstedt LK. Lyme disease. In: Firestein GS, Budd RC, Gabriel SE, McInnes IB, O’Dell JR, editors. Kelley’s Textbook of Rheumatology. 9. Philadelphia: Elsevier Saunders; 2013. pp. 1815–28.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
