

Resource use and costs of type 2 diabetes patients receiving managed or protocolized primary care: a controlled clinical trial
- PMID: 24966055
- PMCID: PMC4099139
- DOI: 10.1186/1472-6963-14-280
Resource use and costs of type 2 diabetes patients receiving managed or protocolized primary care: a controlled clinical trial
Abstract
Background: The increasing prevalence of diabetes is associated with increased health care use and costs. Innovations to improve the quality of care, manage the increasing demand for health care and control the growth of health care costs are needed. The aim of this study is to evaluate the care process and costs of managed, protocolized and usual care for type 2 diabetes patients from a societal perspective.
Methods: In two distinct regions of the Netherlands, both managed and protocolized diabetes care were implemented. Managed care was characterized by centralized organization, coordination, responsibility and centralized annual assessment. Protocolized care had a partly centralized organizational structure. Usual care was characterized by a decentralized organizational structure. Using a quasi-experimental control group pretest-posttest design, the care process (guideline adherence) and costs were compared between managed (n = 253), protocolized (n = 197), and usual care (n = 333). We made a distinction between direct health care costs, direct non-health care costs and indirect costs. Multivariate regression models were used to estimate differences in costs adjusted for confounding factors. Because of the skewed distribution of the costs, bootstrapping methods (5000 replications) with a bias-corrected and accelerated approach were used to estimate 95% confidence intervals (CI) around the differences in costs.
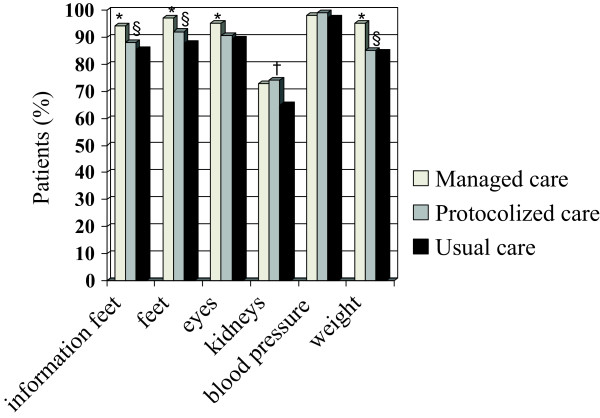
Results: Compared to usual and protocolized care, in managed care more patients were treated according to diabetes guidelines. Secondary health care use was higher in patients under usual care compared to managed and protocolized care. Compared to usual care, direct costs were significantly lower in managed care (€-1.181 (95% CI: -2.597 to -334)) while indirect costs were higher (€ 758 (95% CI: -353 to 2.701), although not significant. Direct, indirect and total costs were lower in protocolized care compared to usual care (though not significantly).
Conclusions: Compared to usual care, managed care was significantly associated with better process in terms of diabetes care, fewer secondary care consultations and lower health care costs. The same trends were seen for protocolized care, however they were not statistically significant.
Trial registration: Current Controlled trials: ISRCTN66124817.
Figures
Similar articles
-
Relationship between glycemic control and diabetes-related hospital costs in patients with type 1 or type 2 diabetes mellitus.J Manag Care Pharm. 2010 May;16(4):264-75. doi: 10.18553/jmcp.2010.16.4.264. J Manag Care Pharm. 2010. PMID: 20433217 Free PMC article.
-
Evaluation of a Pharmacist-Managed Diabetes Program in a Primary Care Setting Within an Integrated Health Care System.J Manag Care Spec Pharm. 2018 Feb;24(2):114-122. doi: 10.18553/jmcp.2018.24.2.114. J Manag Care Spec Pharm. 2018. PMID: 29384029 Free PMC article.
-
Cost-effectiveness of a stepped care program to prevent depression among primary care patients with diabetes mellitus type 2 and/or coronary heart disease and subthreshold depression in comparison with usual care.BMC Psychiatry. 2021 Aug 13;21(1):402. doi: 10.1186/s12888-021-03367-z. BMC Psychiatry. 2021. PMID: 34389017 Free PMC article. Clinical Trial.
-
A comparative study of two various models of organising diabetes follow-up in public primary health care - the model influences the use of services, their quality and costs.BMC Health Serv Res. 2014 Jan 20;14:26. doi: 10.1186/1472-6963-14-26. BMC Health Serv Res. 2014. PMID: 24444378 Free PMC article.
-
Estimated Cost-Effectiveness, Cost Benefit, and Risk Reduction Associated with an Endocrinologist-Pharmacist Diabetes Intense Medical Management "Tune-Up" Clinic.J Manag Care Spec Pharm. 2017 Mar;23(3):318-326. doi: 10.18553/jmcp.2017.23.3.318. J Manag Care Spec Pharm. 2017. PMID: 28230459 Free PMC article.
Cited by
-
Risk stratification by endocrinologists of patients with type 2 diabetes in a Danish specialised outpatient clinic: a cross-sectional study.BMC Health Serv Res. 2016 Apr 9;16:124. doi: 10.1186/s12913-016-1365-y. BMC Health Serv Res. 2016. PMID: 27061722 Free PMC article.
-
How do individuals with alcohol problems use social and healthcare services in Finland? Comparison of service use patterns between two high-need patient groups.Nordisk Alkohol Nark. 2021 Oct;38(5):450-465. doi: 10.1177/14550725211018593. Epub 2021 Jun 8. Nordisk Alkohol Nark. 2021. PMID: 35308819 Free PMC article.
-
Salutogenic model of health to identify turning points and coping styles for eating practices in type 2 diabetes mellitus.Int J Equity Health. 2020 Jun 1;19(1):80. doi: 10.1186/s12939-020-01194-4. Int J Equity Health. 2020. PMID: 32487086 Free PMC article.
-
Defining High Value Elements for Reducing Cost and Utilization in Patient-Centered Medical Homes for the TOPMED Trial.EGEMS (Wash DC). 2019 May 3;7(1):20. doi: 10.5334/egems.246. EGEMS (Wash DC). 2019. PMID: 31106226 Free PMC article.
-
Multimorbidity, health care utilization and costs in an elderly community-dwelling population: a claims data based observational study.BMC Health Serv Res. 2015 Jan 22;15:23. doi: 10.1186/s12913-015-0698-2. BMC Health Serv Res. 2015. PMID: 25609174 Free PMC article.
References
-
- Gruber J. The cost implications of health care reform. N Engl J Med. 2010;14:2050–2051. - PubMed
-
- Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness. JAMA. 2002;14:1775–1779. - PubMed
-
- Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, Part 2. JAMA. 2002;14:1909–1914. - PubMed
-
- Bodenheimer T. The future of primary care: transforming practice. N Engl J Med. 2008;14:2086–2089. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
