

Estimation of the standardized risk difference and ratio in a competing risks framework: application to injection drug use and progression to AIDS after initiation of antiretroviral therapy
- PMID: 24966220
- PMCID: PMC4325676
- DOI: 10.1093/aje/kwu122
Estimation of the standardized risk difference and ratio in a competing risks framework: application to injection drug use and progression to AIDS after initiation of antiretroviral therapy
Abstract
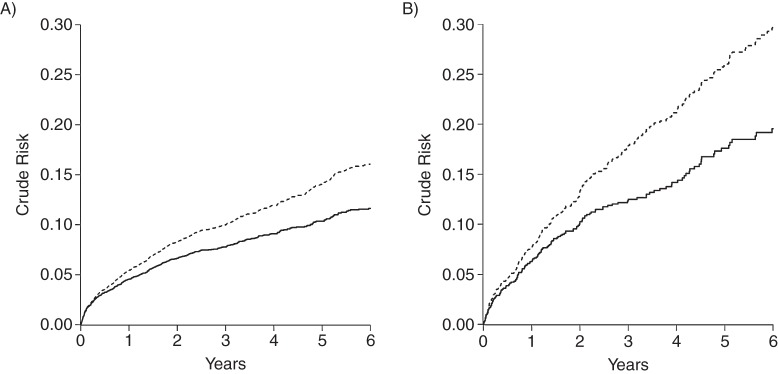
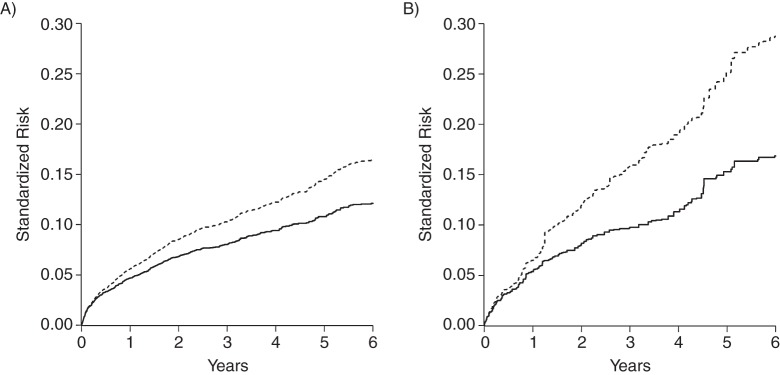
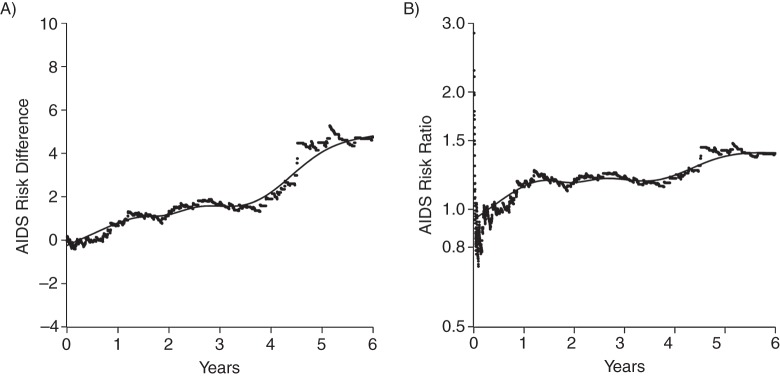
There are few published examples of absolute risk estimated from epidemiologic data subject to censoring and competing risks with adjustment for multiple confounders. We present an example estimating the effect of injection drug use on 6-year risk of acquired immunodeficiency syndrome (AIDS) after initiation of combination antiretroviral therapy between 1998 and 2012 in an 8-site US cohort study with death before AIDS as a competing risk. We estimate the risk standardized to the total study sample by combining inverse probability weights with the cumulative incidence function; estimates of precision are obtained by bootstrap. In 7,182 patients (83% male, 33% African American, median age of 38 years), we observed 6-year standardized AIDS risks of 16.75% among 1,143 injection drug users and 12.08% among 6,039 nonusers, yielding a standardized risk difference of 4.68 (95% confidence interval: 1.27, 8.08) and a standardized risk ratio of 1.39 (95% confidence interval: 1.12, 1.72). Results may be sensitive to the assumptions of exposure-version irrelevance, no measurement bias, and no unmeasured confounding. These limitations suggest that results be replicated with refined measurements of injection drug use. Nevertheless, estimating the standardized risk difference and ratio is straightforward, and injection drug use appears to increase the risk of AIDS.
Keywords: AIDS; HIV; cohort study; competing risks; survival function.
© The Author 2014. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Greenland S. Model-based estimation of relative risks and other epidemiologic measures in studies of common outcomes and in case-control studies. Am J Epidemiol. 2004;160(4):301–305. - PubMed
-
- Robins JM, Morgenstern H. The foundations of confounding in epidemiology. Comput Math Appl. 1987;14(9-12):869–916.
-
- Greenland S. Absence of confounding does not correspond to collapsibility of the rate ratio or rate difference. Epidemiology. 1996;7(5):498–501. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
