

Effect of alveolar ridge preservation after tooth extraction: a systematic review and meta-analysis
- PMID: 24966231
- PMCID: PMC4293706
- DOI: 10.1177/0022034514541127
Effect of alveolar ridge preservation after tooth extraction: a systematic review and meta-analysis
Abstract
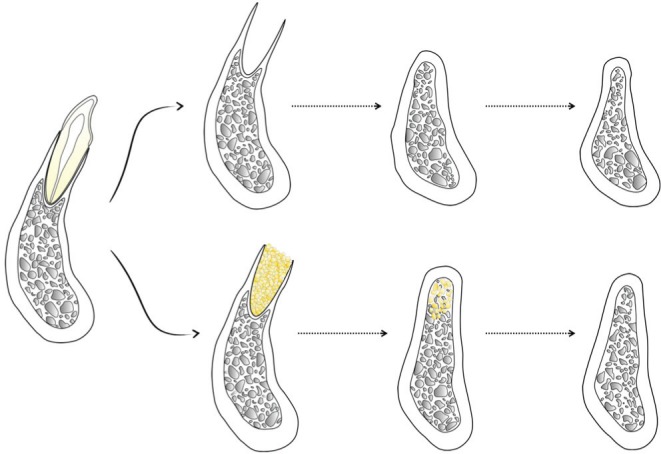
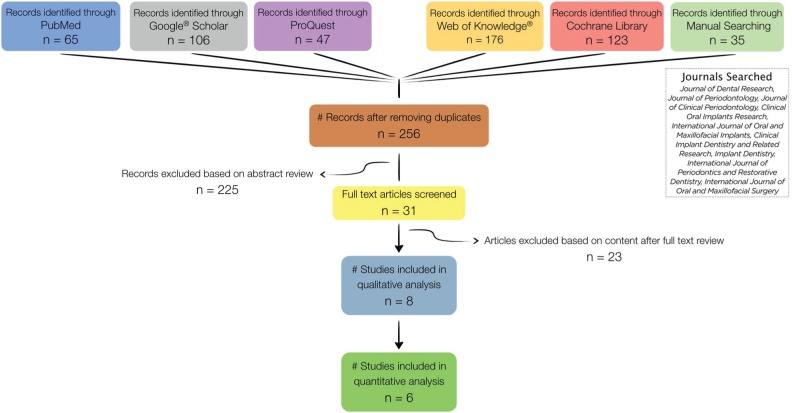
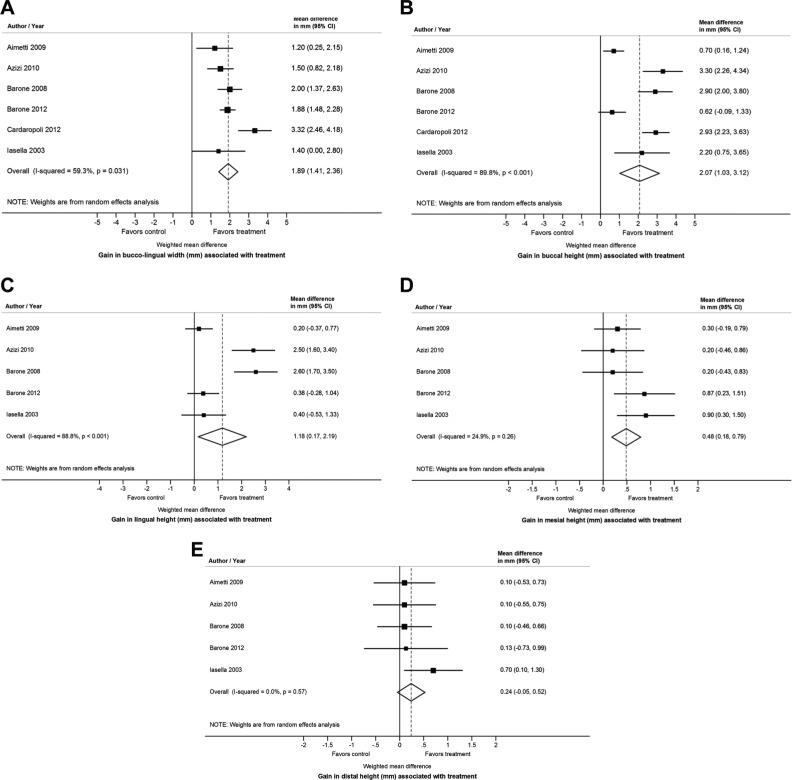
Alveolar ridge preservation strategies are indicated to minimize the loss of ridge volume that typically follows tooth extraction. The aim of this systematic review was to determine the effect that socket filling with a bone grafting material has on the prevention of postextraction alveolar ridge volume loss as compared with tooth extraction alone in nonmolar teeth. Five electronic databases were searched to identify randomized clinical trials that fulfilled the eligibility criteria. Literature screening and article selection were conducted by 3 independent reviewers, while data extraction was performed by 2 independent reviewers. Outcome measures were mean horizontal ridge changes (buccolingual) and vertical ridge changes (midbuccal, midlingual, mesial, and distal). The influence of several variables of interest (i.e., flap elevation, membrane usage, and type of bone substitute employed) on the outcomes of ridge preservation therapy was explored via subgroup analyses. We found that alveolar ridge preservation is effective in limiting physiologic ridge reduction as compared with tooth extraction alone. The clinical magnitude of the effect was 1.89 mm (95% confidence interval [CI]: 1.41, 2.36; p < .001) in terms of buccolingual width, 2.07 mm (95% CI: 1.03, 3.12; p < .001) for midbuccal height, 1.18 mm (95% CI: 0.17, 2.19; p = .022) for midlingual height, 0.48 mm (95% CI: 0.18, 0.79; p = .002) for mesial height, and 0.24 mm (95% CI: -0.05, 0.53; p = .102) for distal height changes. Subgroup analyses revealed that flap elevation, the usage of a membrane, and the application of a xenograft or an allograft are associated with superior outcomes, particularly on midbuccal and midlingual height preservation.
Keywords: alveolar bone atrophy; alveolar bone grafting; alveolar bone loss; bone remodeling; evidence-based dentistry; tooth loss.
© International & American Associations for Dental Research.
Conflict of interest statement
The author(s) received no financial support and declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures
Comment in
-
Alveolar ridge preservation with bone graft may limit physiological ridge loss after tooth extraction.J Am Dent Assoc. 2016 Mar;147(3):204-6. doi: 10.1016/j.adaj.2015.12.015. Epub 2016 Jan 8. J Am Dent Assoc. 2016. PMID: 26775138 No abstract available.
References
-
- Aimetti M, Romano F, Griga FB, Godio L. (2009). Clinical and histologic healing of human extraction sockets filled with calcium sulfate. Int J Oral Maxillofac Implants 24:902-909. - PubMed
-
- Araujo MG, Lindhe J. (2009). Ridge alterations following tooth extraction with and without flap elevation: an experimental study in the dog. Clin Oral Implants Res 20:545-549. - PubMed
-
- Artzi Z, Nemcovsky CE. (1998). The application of deproteinized bovine bone mineral for ridge preservation prior to implantation: clinical and histological observations in a case report. Journal of periodontology 69:1062-1067. - PubMed
-
- Azizi A, Moghadam SA. (2009). A study on the effect of Bio-Oss and collagen membrane on the repair of dental socket. Journal of Isfahan Dental School 5:133-139.
-
- Barone A, Aldini NN, Fini M, Giardino R, Calvo Guirado JL, Covani U. (2008). Xenograft versus extraction alone for ridge preservation after tooth removal: a clinical and histomorphometric study. J Periodontol 79:1370-1377. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
