Nonamplified FGFR1 is a growth driver in malignant pleural mesothelioma
- PMID: 24966347
- PMCID: PMC4201974
- DOI: 10.1158/1541-7786.MCR-14-0038
Nonamplified FGFR1 is a growth driver in malignant pleural mesothelioma
Abstract
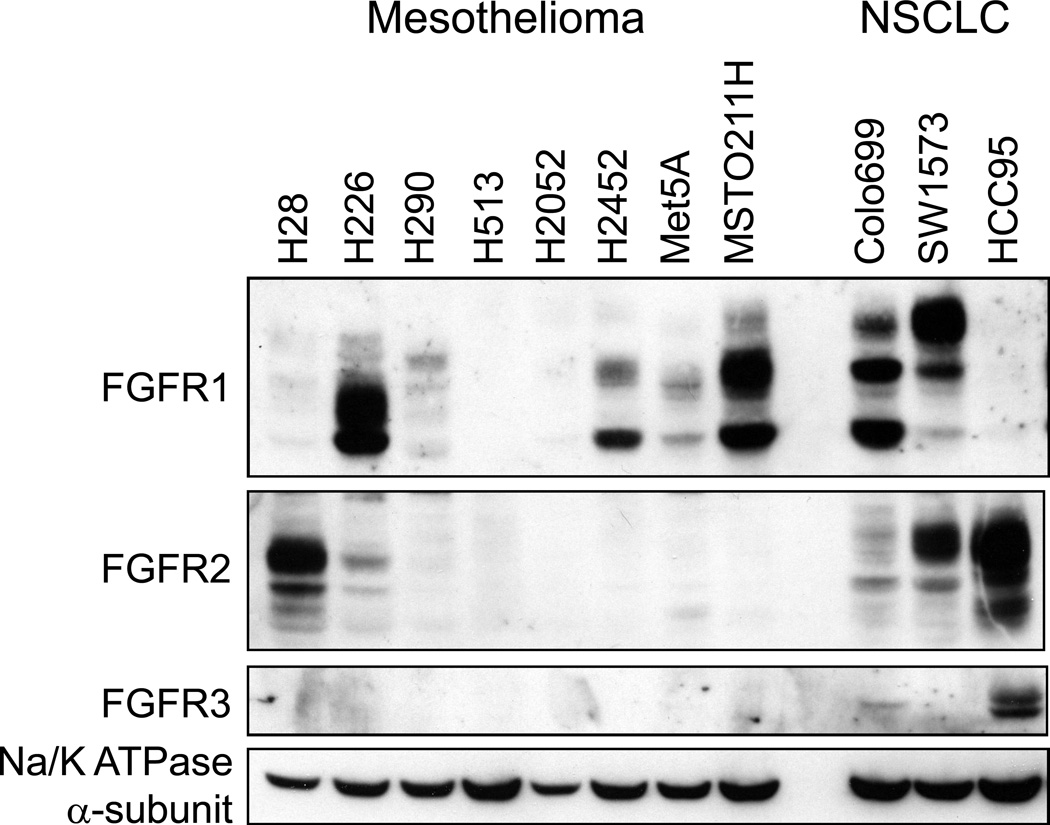
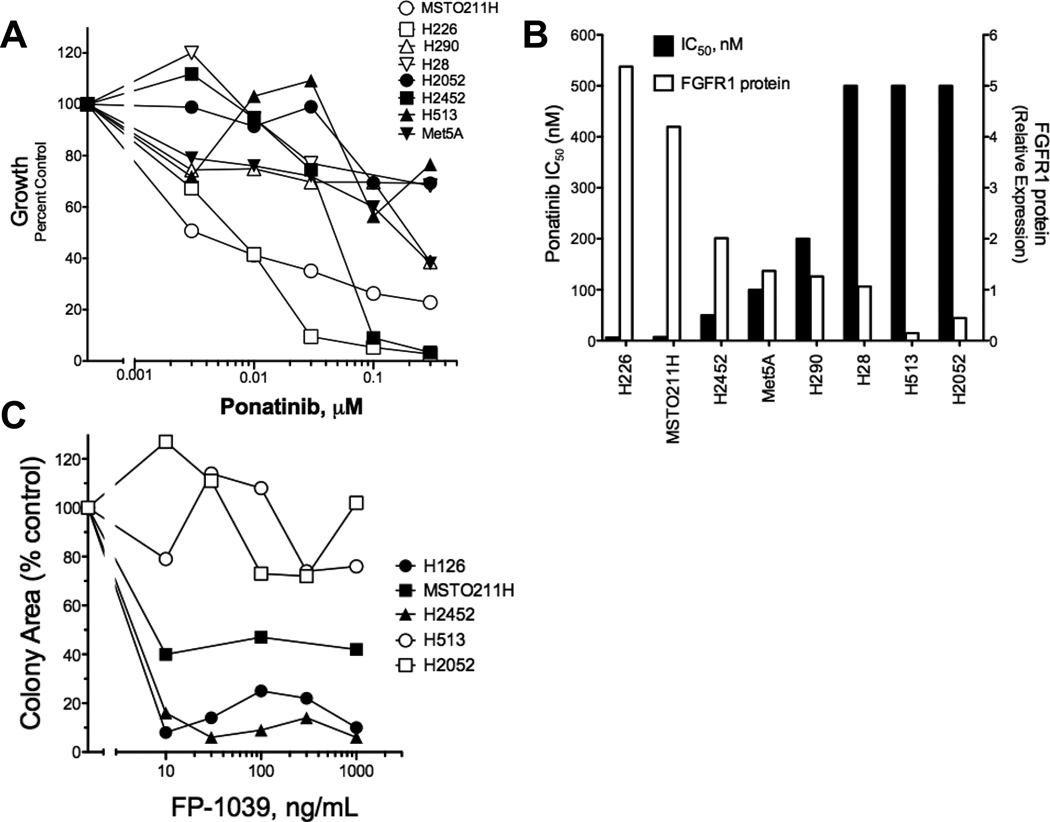
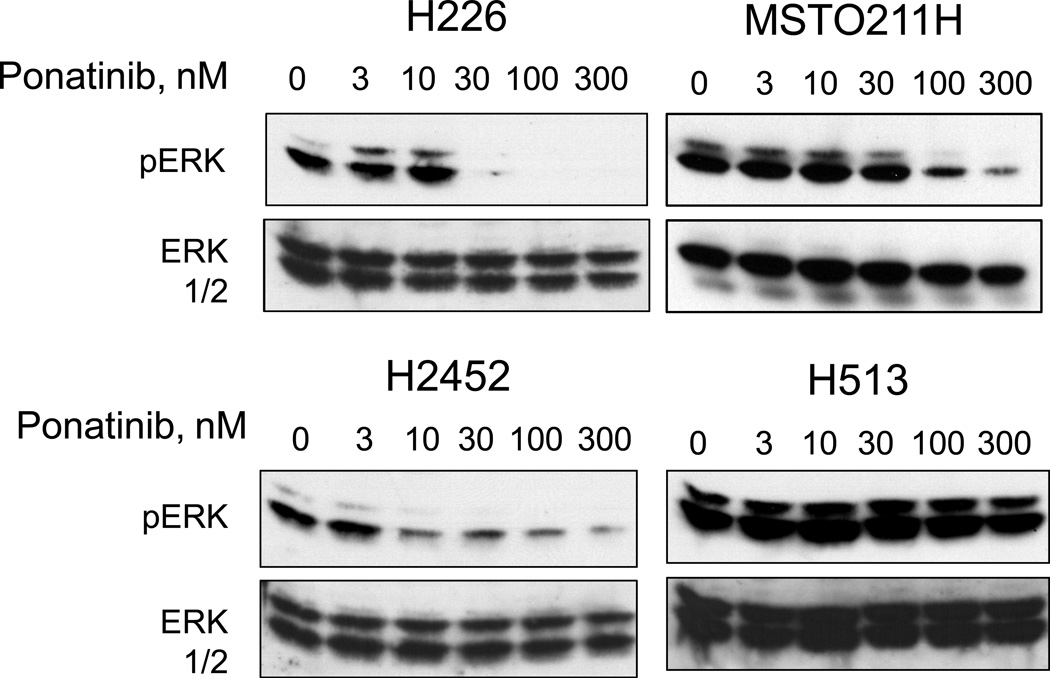
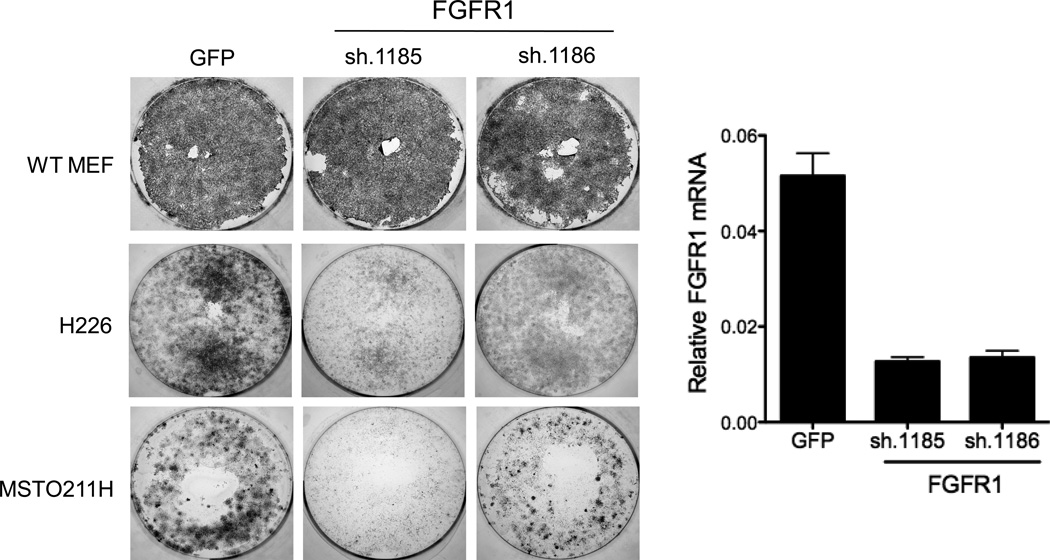
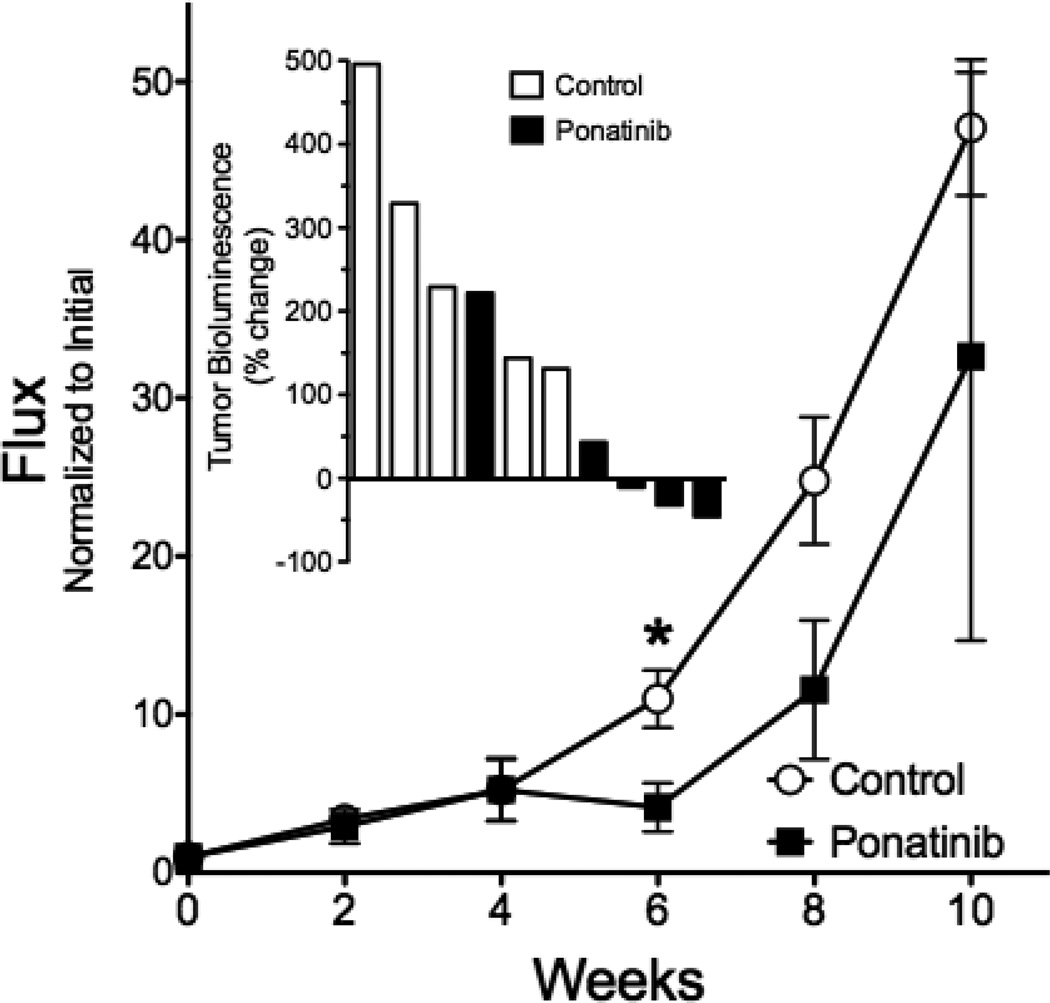
Malignant pleural mesothelioma (MPM) is associated with asbestos exposure and is a cancer that has not been significantly affected by small molecule-based targeted therapeutics. Previously, we demonstrated the existence of functional subsets of lung cancer and head and neck squamous cell carcinoma (HNSCC) cell lines in which fibroblast growth factor receptor (FGFR) autocrine signaling functions as a nonmutated growth pathway. In a panel of pleural mesothelioma cell lines, FGFR1 and FGF2 were coexpressed in three of seven cell lines and were significantly associated with sensitivity to the FGFR-active tyrosine kinase inhibitor (TKI), ponatinib, both in vitro and in vivo using orthotopically propagated xenografts. Furthermore, RNAi-mediated silencing confirmed the requirement for FGFR1 in specific mesothelioma cells and sensitivity to the FGF ligand trap, FP-1039, validated the requirement for autocrine FGFs. None of the FGFR1-dependent mesothelioma cells exhibited increased FGFR1 gene copy number, based on a FISH assay, indicating that increased FGFR1 transcript and protein expression were not mediated by gene amplification. Elevated FGFR1 mRNA was detected in a subset of primary MPM clinical specimens and like MPM cells; none harbored increased FGFR1 gene copy number. These results indicate that autocrine signaling through FGFR1 represents a targetable therapeutic pathway in MPM and that biomarkers distinct from increased FGFR1 gene copy number such as FGFR1 mRNA would be required to identify patients with MPM bearing tumors driven by FGFR1 activity.
Implications: FGFR1 is a viable therapeutic target in a subset of MPMs, but FGFR TKI-responsive tumors will need to be selected by a biomarker distinct from increased FGFR1 gene copy number, possibly FGFR1 mRNA or protein levels.
©2014 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Raja S, Murthy SC, Mason DP. Malignant pleural mesothelioma. Curr Oncol Rep. 2011;13:259–264. - PubMed
-
- Becklake MR, Bagatin E, Neder JA. Asbestos-related diseases of the lungs and pleura: uses, trends and management over the last century. Int J Tuberc Lung Dis. 2007;11:356–369. - PubMed
-
- Ceresoli GL, Locati LD, Ferreri AJ, Cozzarini C, Passoni P, Melloni G, et al. Therapeutic outcome according to histologic subtype in 121 patients with malignant pleural mesothelioma. Lung Cancer. 2001;34:279–287. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous