

The accuracy of computer-assisted primary mandibular reconstruction with vascularized bone flaps: iliac crest bone flap versus osteomyocutaneous fibula flap
- PMID: 24966700
- PMCID: PMC4064953
- DOI: 10.2147/MDER.S62698
The accuracy of computer-assisted primary mandibular reconstruction with vascularized bone flaps: iliac crest bone flap versus osteomyocutaneous fibula flap
Abstract
Background: The intention of mandibular reconstruction is to restore the complex anatomy with maximum possible functionality and high accuracy. The aim of this study was to evaluate the accuracy of computer-assisted surgery in primary mandibular reconstruction with an iliac crest bone flap compared with an osteomyocutaneous fibula flap.
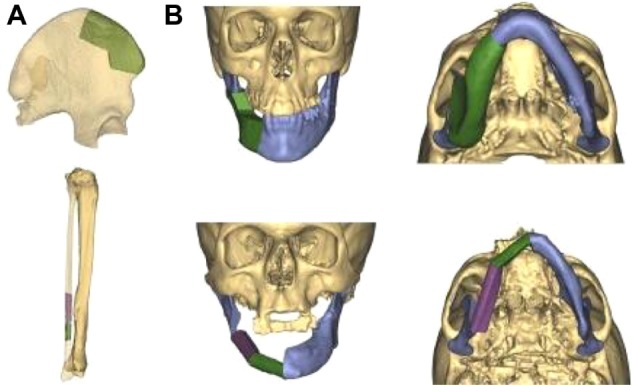
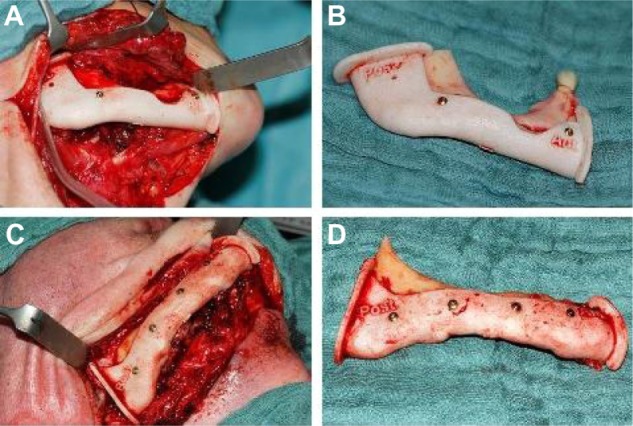
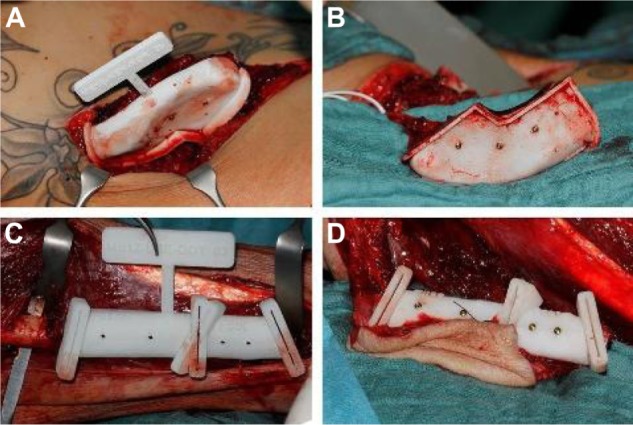
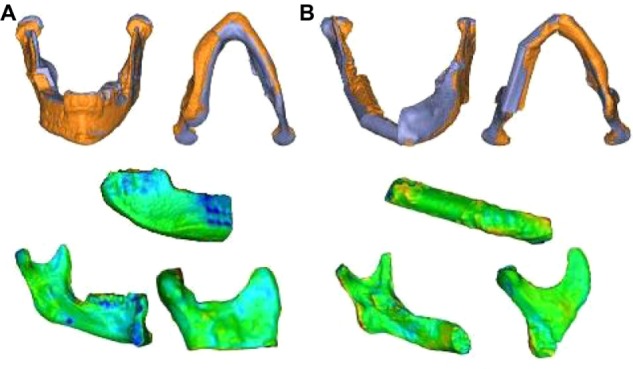
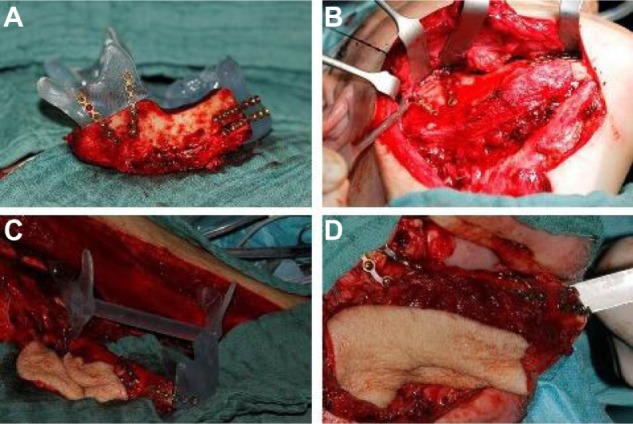
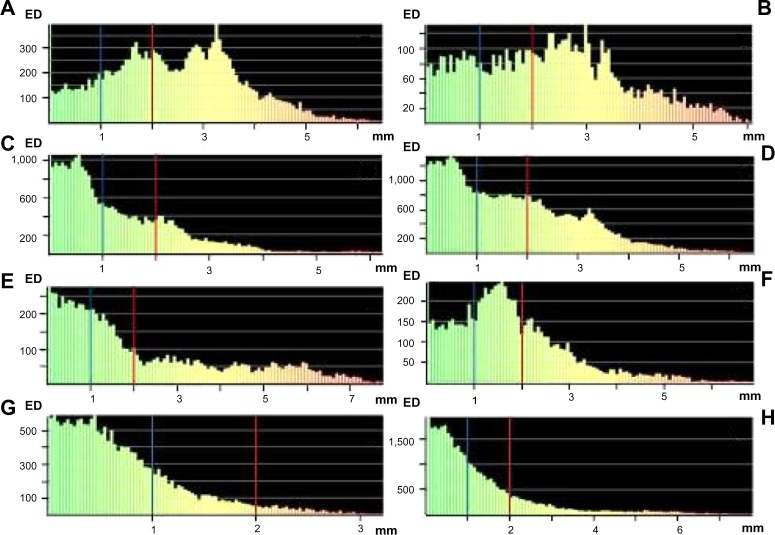
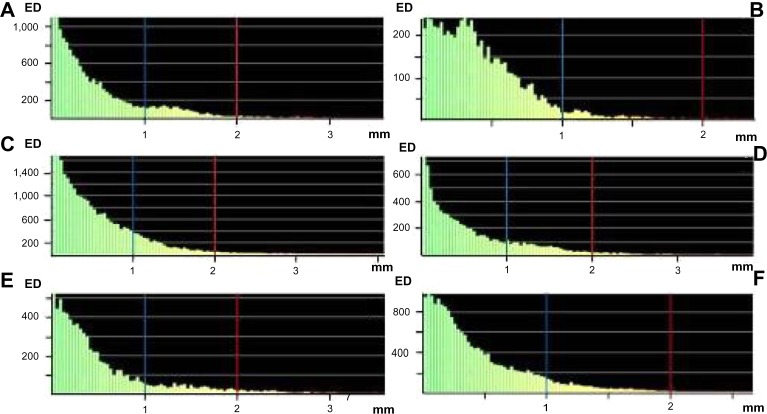
Materials and methods: Preoperative computed tomography data of the mandible and the iliac crest or fibula donor site were imported into a specific surgical planning software program. Surgical guides were manufactured using a rapid prototyping technique for translating the virtual plan, including information on the transplant dimensions and shape, into real-time surgery. Using postoperative computed tomography scans and an automatic surface-comparison algorithm, the actual postoperative situation was compared with the preoperative virtual simulation.
Results: The actual flap position showed a mean difference from the virtual plan of 2.43 mm (standard deviation [SD] ±1.26) and a surface deviation of 39% <2 mm and 15% <1 mm for the iliac crest bone flap, and a mean difference of 2.18 mm (SD ±1.93) and a surface deviation of 60% <2 mm and 37% <1 mm for the osteomyocutaneous fibula flap. The position of the neomandible reconstructed with an osteomyocutaneous fibula flap indicated a mean difference from the virtual plan of 1.25 mm (SD ±1.31) and a surface deviation of 82% <2 mm and 57% <1 mm, in contrast to a mean difference of 1.68 mm (SD ±1.25) and a surface deviation of 63% <2 mm and 38% <1 mm for the neomandible after reconstruction with an iliac crest bone flap. For shape analysis, a similarly high accuracy could be calculated for both flaps.
Conclusion: Virtual surgical planning is an effective method for mandibular reconstruction with vascularized bone flaps, and can help to restore the anatomy of the mandible with high accuracy in position and shape. It seems that primary mandibular reconstruction with the osteomyocutaneous fibula flap is more accurate compared with the vascularized iliac crest bone flap.
Keywords: computer-assisted surgery; primary mandibular reconstruction; surgical guide; vascularized bone flaps; virtual planning.
Figures
References
-
- Chow JM, Hill JH. Primary mandibular reconstruction using the AO reconstruction plate. Laryngoscope. 1986;96:768–773. - PubMed
-
- Leake DL, Rappoport M. Mandibular reconstruction: bone induction in an alloplastic tray. Surgery. 1972;72:332–336. - PubMed
-
- Cordeiro PG, Disa JJ, Hidalgo DA, Hu QY. Reconstruction of the mandible with osseous free flaps: a 10-year experience with 150 consecutive patients. Plast Reconstr Surg. 1999;104:1314–1320. - PubMed
-
- Disa JJ, Cordeiro PG. Mandible reconstruction with microvascular surgery. Semin Surg Oncol. 2000;19:226–234. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
