

A case of recurrent autoimmune hemolytic anemia during remission associated with acute pure red cell aplasia and hemophagocytic syndrome due to human parvovirus B19 infection successfully treated by steroid pulse therapy with a review of the literature
- PMID: 24966977
- PMCID: PMC4069955
A case of recurrent autoimmune hemolytic anemia during remission associated with acute pure red cell aplasia and hemophagocytic syndrome due to human parvovirus B19 infection successfully treated by steroid pulse therapy with a review of the literature
Abstract
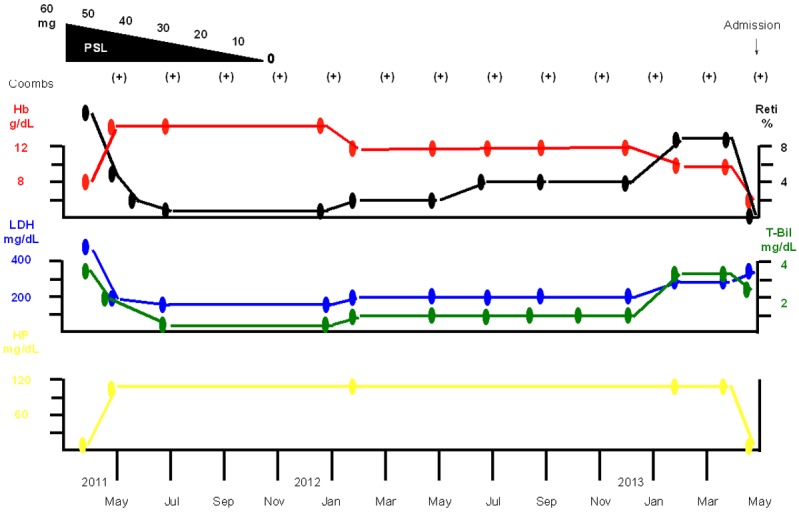
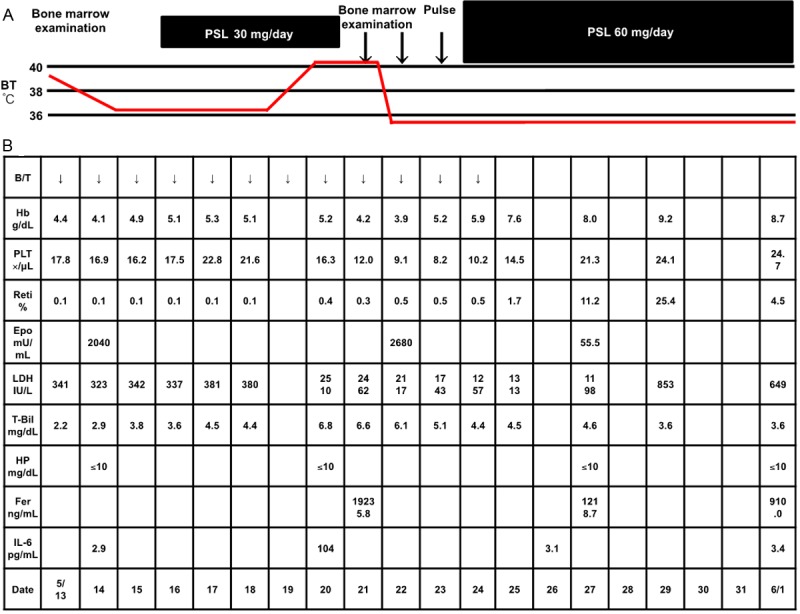
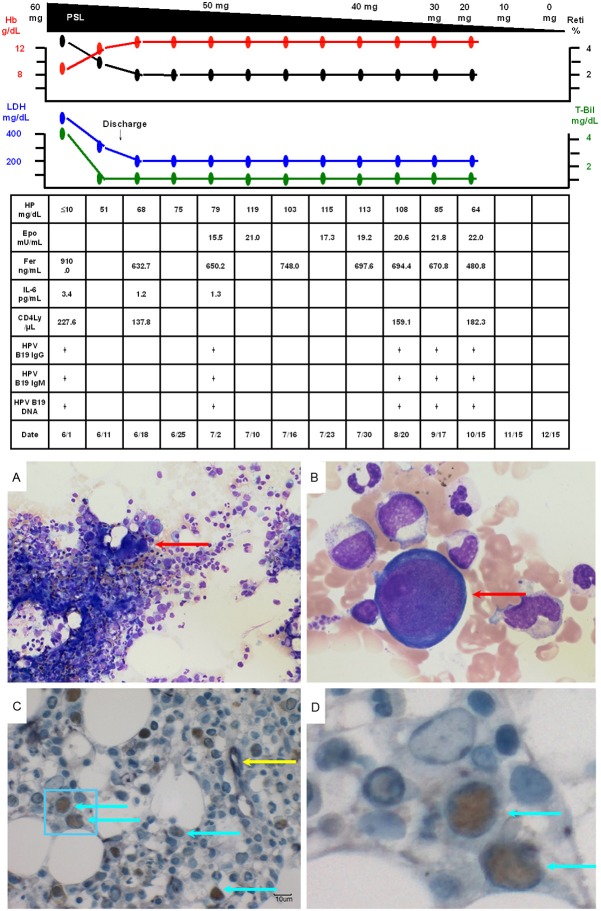
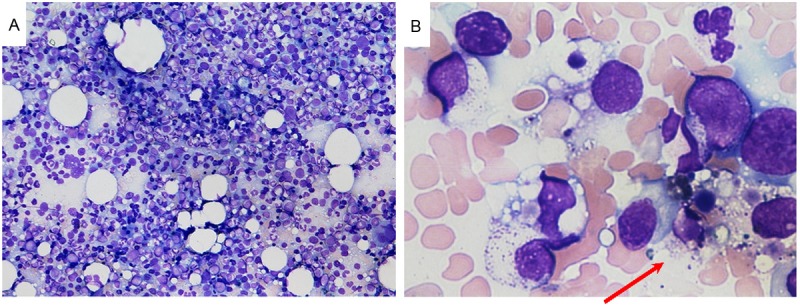
The patient was a 47-year-old man diagnosed as having autoimmune hemolytic anemia (AIHA) in April 2011. He also had a congenital chromosomal abnormality, a balanced translocation. Treatment with prednisolone (PSL) 60 mg/day resulted in resolution of the AIHA, and the treatment was completed in November 2011. While the patient no longer had anemia, the direct and indirect Coombs tests remained positive. In May 2013, he developed recurrent AIHA associated with acute pure red cell aplasia (PRCA) and hemophagocytic syndrome (HPS) caused by human parvovirus B19 (HPV B19) infection. Tests for anti-erythropoietin and anti-erythropoietin receptor antibodies were positive. Steroid pulse therapy resulted in resolution of the AIHA, PRCA, as well as HPS. The serum test for anti-erythropoietin antibodies also became negative after the treatment. However, although the serum was positive for anti-HPV B19 IgG antibodies, the patient continued to have a low CD4 lymphocyte count (CD4, <300/μL) and persistent HPV B19 infection (HPV B19 DNA remained positive), suggesting the risk of recurrence and bone marrow failure.
Keywords: Autoimmune hemolytic anemia; CD4 lymphocyte count; hemophagocytic syndrome; human parvovirus B19; pure red cell aplasia.
Figures
References
-
- Eisemann G, Dameshek W. Splenectomy for pure red-cell hypoplastic (aregenerative) anemia associated with autoimmune hemolytic disease; report of a case. N Engl J Med. 1954;251:1044–1048. - PubMed
-
- Seip M. Aplastic crisis in a case of immuno-hemolytic anemia. Acta Med Scand. 1955;153:137–42. - PubMed
-
- Bove JR. Combined erythroid hypoplasia and symptomatic hemolytic anemia; report of a case. N Engl J Med. 1956;255:135–136. - PubMed
-
- Hennemann HH, Falck I. [Combinations of aplastic with hemolytic syndromes] . Acta Haematol. 1957;18:219–228. German. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous