

Adrenal and extra-adrenal myelolipomas - a comparative case report
- PMID: 24967008
- PMCID: PMC4037239
- DOI: 10.3941/jrcr.v8i1.1551
Adrenal and extra-adrenal myelolipomas - a comparative case report
Abstract
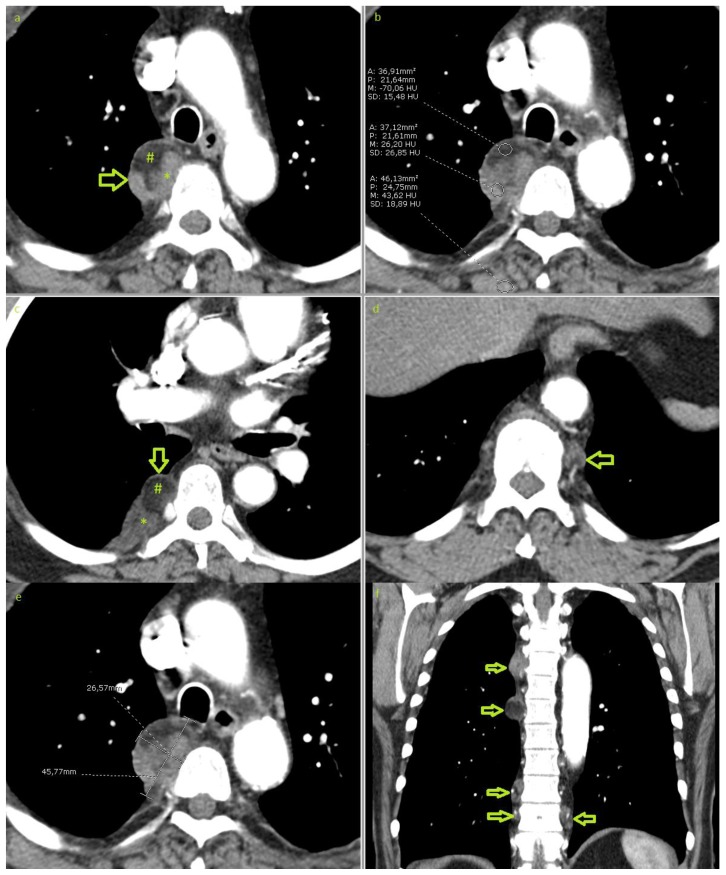
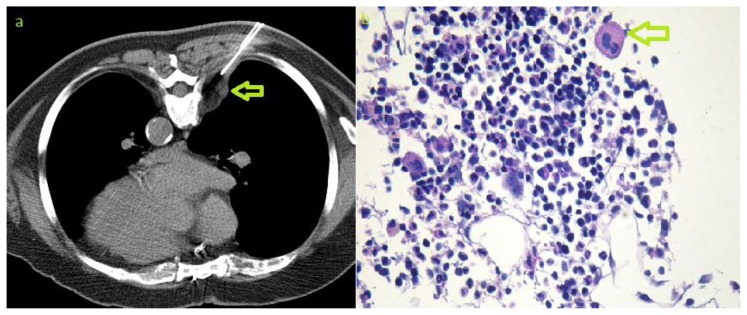
Myelolipoma is an uncommon benign tumour composed of mature fat tissue and haematopoietic elements and is most commonly found in the adrenal gland. We report a case, which was discovered incidentally on chest X-ray, of a rare occurrence of multifocal extra-adrenal myelolipoma in the thoracic paravertebral region. This was further investigated with multi-detector computed tomography and magnetic resonance imaging. The presumed diagnosis, of extra-adrenal myelolipoma, was histologically confirmed via tissue sample obtained by computed tomography guided biopsy. We compare the adrenal and extra-adrenal entities from the perspective of published literature and also review the cases, published in Pubmed, of extra-adrenal myelolipomas in order to summarize the different locations of this lesion.
Keywords: CT; Extra-adrenal; MRI; adrenal; fat; incidental; myelolipoma; paravertebral.
Figures



References
-
- Federle M, Anne V. Adrenal Myelolipoma. In: Federle M, editor. Diagnostic Imaging: Abdomen. 1st ed. Salt lake: Amirsys; 2004. pp. III 2 24–25.
-
- Gierke E. Uber Knochenmarksgewebe in der Nebenniere. Beitr Pathol Anat. 1905;7:311–25.
-
- Oberling C. Les formation myelo-lipomateuses. Bull Assoc Fr Etud Cancer. 1929;18:234–246.
-
- Rao P, Kenney PJ, Wagner BJ, Davidson AJ. Imaging and pathologic features of myelolipoma. Radiographics. 1997 Nov-Dec;17(6):1373–85. - PubMed
-
- Arzanian MT, Khaleghnejad-Tabari A, Shamsian BS, Jadali F, Gharib A, Esfahani H. Generalized myelolipoma. Arch Iran Med. 2006 Jul;9(3):274–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical