

Testicular adrenal rest tumors in a patient with congenital adrenal hyperplasia
- PMID: 24967019
- PMCID: PMC4037253
- DOI: 10.3941/jrcr.v8i2.1489
Testicular adrenal rest tumors in a patient with congenital adrenal hyperplasia
Abstract
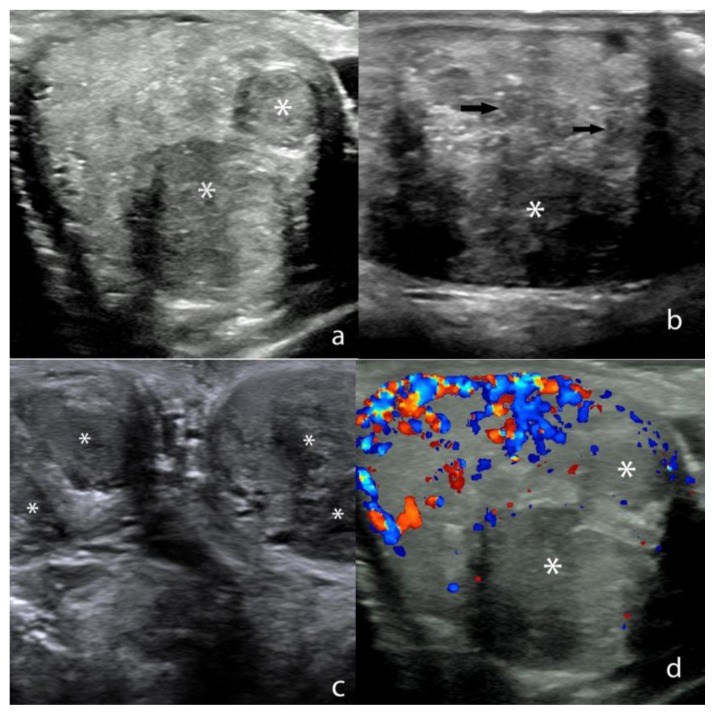
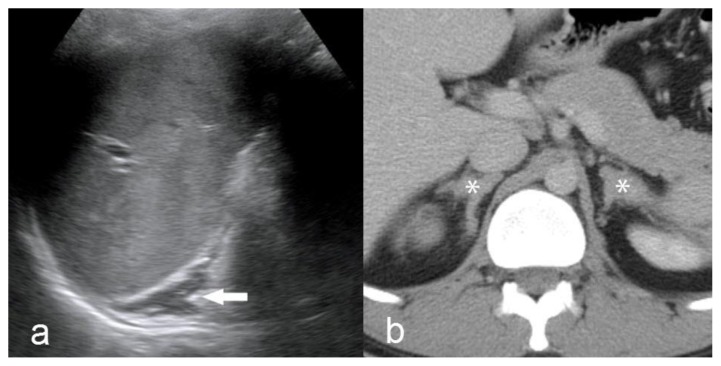
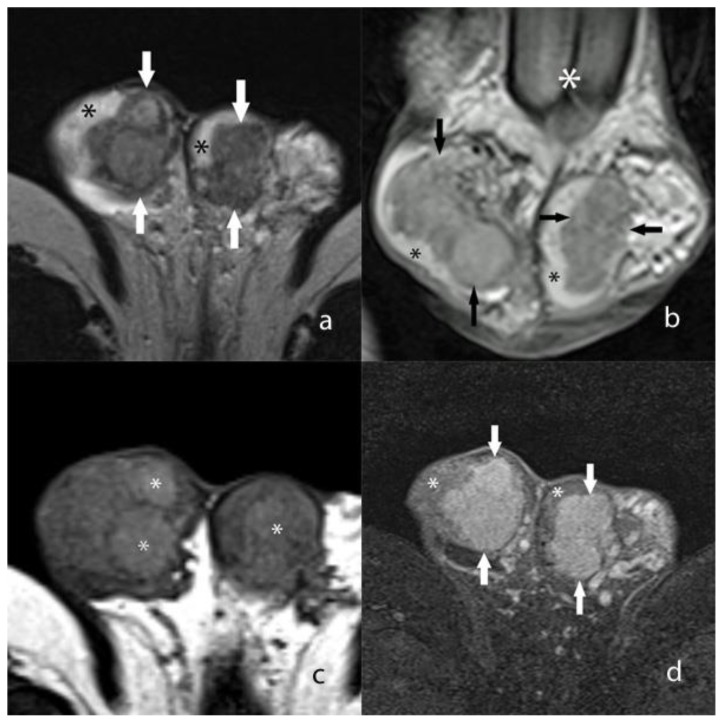
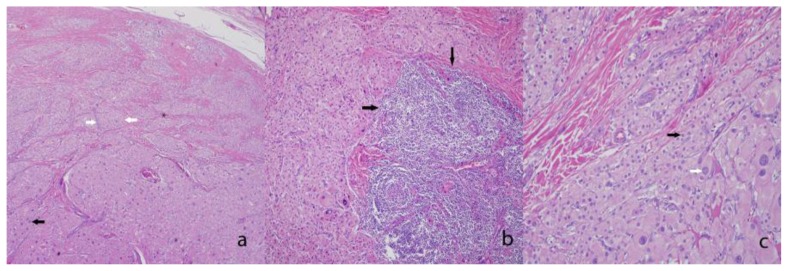
Congenital adrenal hyperplasia refers to a group of autosomal recessive disorders caused by a deficiency of an enzyme involved in the synthesis of glucocorticoids. The enzyme deficiency generally leads to a deficiency of cortisol and/or aldosterone production within the adrenal cortex. The lack of glucocorticoids generally leads to elevated levels of plasma corticotropin (ACTH), which often results in adrenal hyperplasia. Testicular adrenal rest tumors may develop in males with congenital adrenal hyperplasia due to overstimulation of aberrant adrenal cells within the testes. Recognition of this disease entity is essential when evaluating young males with testicular masses.
Keywords: Congenital adrenal hyperplasia; testicular adrenal rest tumors; testicular ultrasonography.
Figures
References
-
- Speiser PW, White PC. Congenital adrenal hyperplasia. The New England journal of medicine. 2003;349(8):776–788. - PubMed
-
- Therrell BL, Jr, Berenbaum SA, Manter-Kapanke V, Simmank J, Korman K, Prentice L, Gonzalez J, Gunn S. Results of screening 1.9 million Texas newborns for 21-hydroxylase-deficient congenital adrenal hyperplasia. Pediatrics. 1998;101(4 Pt 1):583–590. - PubMed
-
- Wilkins L. Macrogenitosomia precox associated with hyperplasia of the androgenic tissue of the adrenal and death from corticoadrenal insufficiency. Endocrinology. 1940;26:385–395.
-
- Avila NA, Shawker TS, Jones JV, Cutler GB, Jr, Merke DP. Testicular adrenal rest tissue in congenital adrenal hyperplasia: serial sonographic and clinical findings. AJR American journal of roentgenology. 1999;172(5):1235–1238. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical