

Intercostal lung herniation--the role of imaging
- PMID: 24967031
- PMCID: PMC4035464
- DOI: 10.3941/jrcr.v8i4.1606
Intercostal lung herniation--the role of imaging
Abstract
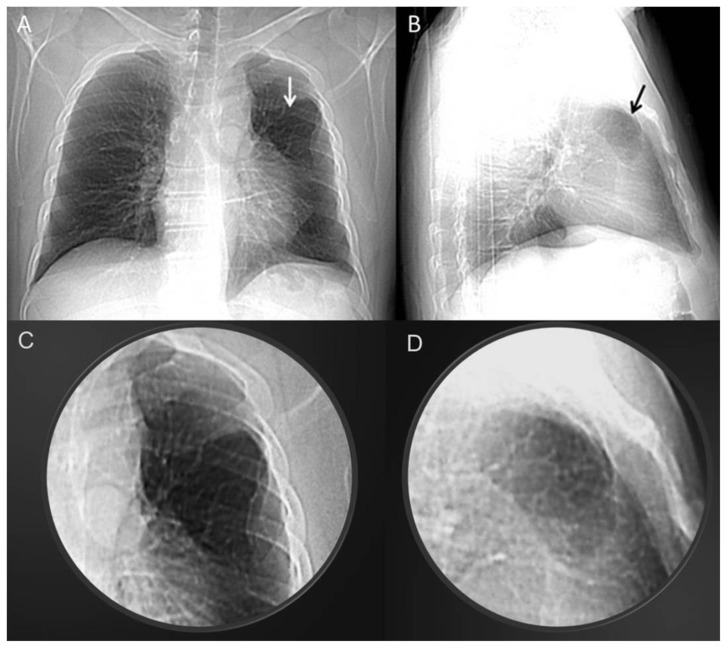
Extrathoracic lung hernias can be congenital or acquired. Acquired hernias may be classified by etiology into traumatic, spontaneous, and pathologic. We present a case of a 40-year-old male with a history of bronchial asthma and a blunt chest trauma who presented complaining of sharp chest pain of acute onset that began after five consecutive days of vigorous coughing. Upon physical examination a well-demarcated deformity overlying the third intercostal space of the left upper anterior hemithorax was revealed. Thoracic CT scan showed that a portion of the anterior bronchopulmonary segment of the left upper lobe had herniated through a chest wall defect. The role of imaging, especially chest computed tomography with multiplanar image reconstructions and maximum (MIP) and minimum intensity projection (MinIP) reformats can clearly confirm the presence of the herniated lung, the hernial sac, the hernial orifice in the chest wall, and exclude possible complications such as lung tissue strangulation.
Keywords: Intercostal lung hernia; computed tomography; image reformats.
Figures





Similar articles
-
[Traumatic intercostal pulmonary hernia; report of a case].Kyobu Geka. 2008 Jun;61(6):504-7. Kyobu Geka. 2008. PMID: 18536303 Japanese.
-
The image of trauma. Transthoracic lung herniation due to blunt trauma.J Trauma. 2006 May;60(5):1149. doi: 10.1097/01.ta.0000201327.73448.42. J Trauma. 2006. PMID: 16688090 No abstract available.
-
[Cough-induced intercostal lung herniation successfully diagnosed with imaging techniques].Recenti Prog Med. 2012 Nov;103(11):523-5. doi: 10.1701/1166.12901. Recenti Prog Med. 2012. PMID: 23096744 Italian.
-
Soft right chest wall swelling simulating lipoma following motor vehicle accident: transdiaphragmatic intercostal hernia. A case report and review of literature.Hernia. 2008 Oct;12(5):539-43. doi: 10.1007/s10029-008-0342-8. Epub 2008 Feb 22. Hernia. 2008. PMID: 18293055 Review.
-
Traumatic thoracic rib cage and chest wall hernias: A review and discussion of management principles.Am J Surg. 2021 Jun;221(6):1238-1245. doi: 10.1016/j.amjsurg.2021.03.024. Epub 2021 Mar 20. Am J Surg. 2021. PMID: 33773751 Review.
Cited by
-
Spontaneous Combined Lung and Bowel Herniation Due to Uncontrolled Asthma.Cureus. 2023 Feb 13;15(2):e34939. doi: 10.7759/cureus.34939. eCollection 2023 Feb. Cureus. 2023. PMID: 36938229 Free PMC article.
-
Lung herniation after positive pressure ventilation.Respir Med Case Rep. 2016 Dec 18;20:61-63. doi: 10.1016/j.rmcr.2016.12.003. eCollection 2017. Respir Med Case Rep. 2016. PMID: 28053853 Free PMC article.
-
Incidental discovery of intercostal pulmonary hernia: A case report.Radiol Case Rep. 2022 Sep 26;17(12):4510-4514. doi: 10.1016/j.radcr.2022.08.068. eCollection 2022 Dec. Radiol Case Rep. 2022. PMID: 36189153 Free PMC article.
-
Intercostal lung herniation secondary to thoracotomy: a case report.Pan Afr Med J. 2020 May 27;36:39. doi: 10.11604/pamj.2020.36.39.20054. eCollection 2020. Pan Afr Med J. 2020. PMID: 32774615 Free PMC article.
-
Spinal cord compression by a pulmonary hernia.Rev Bras Ortop. 2018 Sep 20;53(6):802-804. doi: 10.1016/j.rboe.2018.09.002. eCollection 2018 Nov-Dec. Rev Bras Ortop. 2018. PMID: 30377620 Free PMC article.
References
-
- Donato AT, Hipona FA, Navani S. Spontaneous lung hernia. Chest. 1973 Aug;64(2):254–6. - PubMed
-
- Francois B, Desachy A, Cornu E, Ostyn E, Niquet L, Vignon P. Traumatic pulmonary hernia: surgical versus conservative management. J Trauma. 1998;44:217–9. - PubMed
-
- Morel-Lavallée Hernies du poumon. Bull Soc Chir Paris. 1845–1847;1:75–195.
-
- Hiscoe DB, Digman GJ. Types and incidence of lung hernias. J Thorac Cardiovasc Surg. 1955;30:335–42. - PubMed
-
- Moncada R, Vade A, Gimenez C, Rosado W, Demos TC, Turbin R, Venta L. Congenital and acquired lung hernias. J Thorac Imag. 1996;11:75–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical