

Case Reports
doi: 10.3941/jrcr.v8i4.1572.
eCollection 2014 Apr.
The curious case of the disappearing IVC: a case report and review of the aetiology of inferior vena cava agenesis
Affiliations
- PMID: 24967034
- PMCID: PMC4035467
- DOI: 10.3941/jrcr.v8i4.1572
Item in Clipboard
Case Reports
The curious case of the disappearing IVC: a case report and review of the aetiology of inferior vena cava agenesis
J Radiol Case Rep.
.
Abstract
We report the case of a previously well 18-year-old male who presented to the Emergency Department with lower limb pain. An ultrasound demonstrated extensive left sided deep vein thrombosis and computed tomography demonstrated inferior vena cava agenesis, leading to the diagnosis of inferior vena cava agenesis associated deep vein thrombosis. The aetiology of inferior vena cava agenesis is explored in depth.
Keywords: IVC; Inferior vena cava agenesis; deep vein thrombosis; inferior vena cava agenesis associated deep vein thrombosis; inferior vena cava anomalies; venous thromboembolism.
Figures

18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: Sagittal ultrasound image shows thrombus in the left common iliac vein (green arrow) with good blood flow in the artery overlying. TECHNIQUE: Ultrasonography was performed using a Philips IU22 (Philips Healthcare UK) ultrasound machine with linear array and curvilinear 5 - 2 megahertz (MHz) probes.

18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: Normal posterior-anterior chest radiograph appearances.

18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: Venous phase axial (a) and coronal (b) enhanced computed tomography of the abdomen demonstrating the small right sided suprarenal IVC cava (white arrows; solid white arrow in magnification (b)). TECHNIQUE: The patient was imaged on a Siemens Sensation 16 CT Scanner (Siemens Medical, Forchheim Germany) scanned helically with axial reconstruction at 1.5mms, matrix size 512×512, with 120kVp and modulated mAs varying from 70 to 205. An initial scan was acquired after administration of non ionic Iopamidol (Niopam 300mg Iodine/ml Bracco UK Limited) IV Contrast triggered from the aorta with 25 second delayed imaging performed from pelvis to lung apices with a second study of the pelvis visually triggered over the IVC as initial opacification of pelvic veins was poor. A pump injection was used with a speed of 4 mls/sec. The legs were not imaged as ultrasound had provided diagnostic information regarding the presence of thrombus on the left side.

18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: Coronal views of the abdomen at different levels (a posterior to b) demonstrating a large collateral vessel (white arrows; hollow white arrow in magnification (a)) containing thrombus, draining the right kidney. TECHNIQUE: The patient was imaged on a Siemens Sensation 16 CT Scanner (Siemens Medical, Forchheim Germany) scanned helically with axial reconstruction at 1.5mms, matrix size 512×512, with 120kVp and modulated mAs varying from 70 to 205. An initial scan was acquired after administration of non ionic Iopamidol (Niopam 300mg Iodine/ml Bracco UK Limited) IV Contrast triggered from the aorta with 25 second delayed imaging performed from pelvis to lung apices with a second study of the pelvis visually triggered over the IVC as initial opacification of pelvic veins was poor. A pump injection was used with a speed of 4 mls/sec. The legs were not imaged as ultrasound had provided diagnostic information regarding the presence of thrombus on the left side.

18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: Computed tomography axial scan (a) of the abdomen showing a lumbar vein (blue arrow in main image (a); solid blue arrow in magnification (a)) forming bulbous left ‘inferior vena cava’ (white arrow in main image; solid white arrow in magnification (a)). Coronal image (b) demonstrating a left gonadal vein (blue arrow in main image (b); solid blue arrow in magnification (b)) with left sided collaterals (orange arrow in main image (b); solid orange arrow in magnification (b)) draining into the bulbous left ‘inferior vena cava’ which crosses the aorta to join the suprarenal portion of the right sided inferior vena cava (white arrow in main image (b); solid white arrow in magnification (b)). TECHNIQUE: The patient was imaged on a Siemens Sensation 16 CT Scanner (Siemens Medical, Forchheim Germany) scanned helically with axial reconstruction at 1.5mms, matrix size 512×512, with 120kVp and modulated mAs varying from 70 to 205. An initial scan was acquired after administration of non ionic Iopamidol (Niopam 300mg Iodine/ml Bracco UK Limited) IV Contrast triggered from the aorta with 25 second delayed imaging performed from pelvis to lung apices with a second study of the pelvis visually triggered over the IVC as initial opacification of pelvic veins was poor. A pump injection was used with a speed of 4 mls/sec. The legs were not imaged as ultrasound had provided diagnostic information regarding the presence of thrombus on the left side.

18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: Computed tomography axial scan of the abdomen demonstrating the right sided inferior vena cava (white arrow; solid white arrow in magnification) and left sided collaterals containing thrombus (blue arrow; blue solid arrow in magnification). TECHNIQUE: The patient was imaged on a Siemens Sensation 16 CT Scanner (Siemens Medical, Forchheim Germany) scanned helically with axial reconstruction at 1.5mms, matrix size 512×512, with 120kVp and modulated mAs varying from 70 to 205. An initial scan was acquired after administration of non ionic Iopamidol (Niopam 300mg Iodine/ml Bracco UK Limited) IV Contrast triggered from the aorta with 25 second delayed imaging performed from pelvis to lung apices with a second study of the pelvis visually triggered over the IVC as initial opacification of pelvic veins was poor. A pump injection was used with a speed of 4 mls/sec. The legs were not imaged as ultrasound had provided diagnostic information regarding the presence of thrombus on the left side.
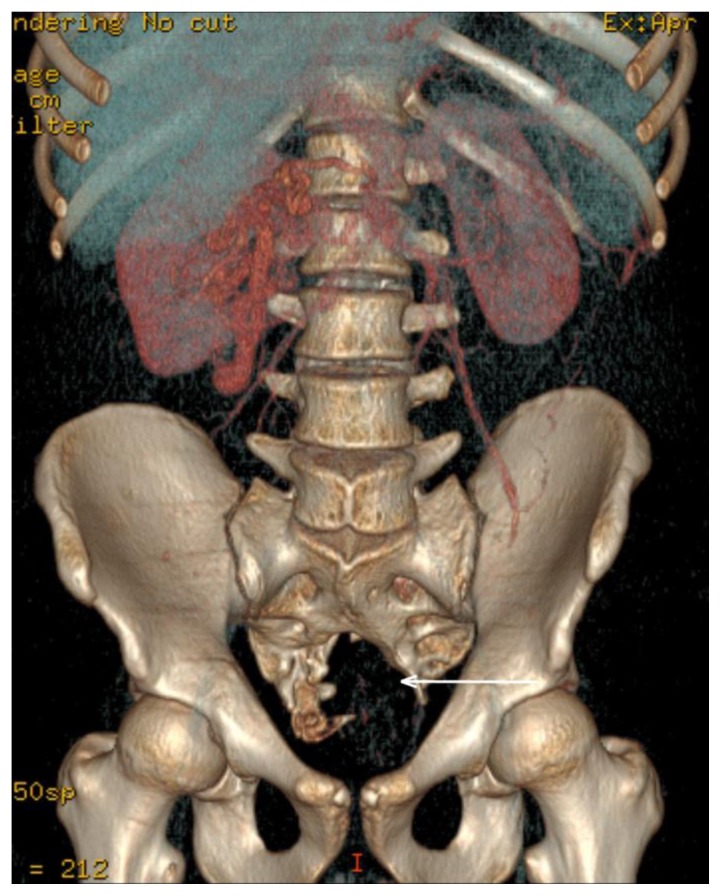
18-year-old male with extensive DVT and infrarenal IVC agenesis. FINDINGS: A three-dimensional volumetric reconstruction demonstrating the left sided sacral bony defect (white arrow). TECHNIQUE: The patient was imaged on a Siemens Sensation 16 CT Scanner (Siemens Medical, Forchheim Germany) scanned helically with axial reconstruction at 1.5mms, matrix size 512×512, with 120kVp and modulated mAs varying from 70 to 205. An initial scan was acquired after administration of non ionic Iopamidol (Niopam 300mg Iodine/ml Bracco UK Limited) IV Contrast triggered from the aorta with 25 second delayed imaging performed from pelvis to lung apices with a second study of the pelvis visually triggered over the IVC as initial opacification of pelvic veins was poor. A pump injection was used with a speed of 4 mls/sec. The legs were not imaged as ultrasound had provided diagnostic information regarding the presence of thrombus on the left side.
Similar articles
-
Deep venous thrombosis in a young woman with hypoplastic inferior vena cava.Ann Vasc Surg. 2014 May;28(4):1036.e5-7. doi: 10.1016/j.avsg.2013.06.044. Epub 2013 Nov 8. Ann Vasc Surg. 2014. PMID: 24216406
-
Thrombolysis for deep venous thrombosis associated with inferior vena cava agenesis in a young patient.BMJ Case Rep. 2019 May 24;12(5):e229840. doi: 10.1136/bcr-2019-229840. BMJ Case Rep. 2019. PMID: 31129644 Free PMC article.
-
Congenital agenesis of inferior vena cava: a rare cause of unprovoked deep venous thrombosis.Ann Vasc Surg. 2015 Jul;29(5):1017.e15-8. doi: 10.1016/j.avsg.2015.01.003. Epub 2015 Mar 6. Ann Vasc Surg. 2015. PMID: 25747887
-
Infrahepatic inferior vena cava agenesis with bilateral renal vein thrombosis.Ann Vasc Surg. 2013 Oct;27(7):973.e19-23. doi: 10.1016/j.avsg.2012.10.030. Ann Vasc Surg. 2013. PMID: 23993114 Review.
-
Endovascular Treatment of Inferior Vena Cava Thrombosis in Metastatic Malignancy: A Case Report and Review of Literature.Vasc Endovascular Surg. 2019 Aug;53(6):507-511. doi: 10.1177/1538574419857992. Epub 2019 Jun 19. Vasc Endovascular Surg. 2019. PMID: 31216954 Review.
Cited by
-
Disappearing Inferior Vena Cava in A Pediatric Patient with Down Syndrome and Hereditary Thrombophilia.J Belg Soc Radiol. 2016 Feb 8;100(1):22. doi: 10.5334/jbr-btr.975. J Belg Soc Radiol. 2016. PMID: 30151445 Free PMC article.
-
Infrarenal inferior vena cava agenesis presenting as acute abdomen and hydronephrosis - case report.Radiol Case Rep. 2023 Jun 22;18(9):3070-3075. doi: 10.1016/j.radcr.2023.06.003. eCollection 2023 Sep. Radiol Case Rep. 2023. PMID: 37434616 Free PMC article.
-
Inferior Vena Cava Agenesis: An Unusual Cause of Deep Vein Thrombosis and Pulmonary Embolism in Young Adult Patients.EJVES Short Rep. 2018 Apr 22;39:12-15. doi: 10.1016/j.ejvssr.2018.03.005. eCollection 2018. EJVES Short Rep. 2018. PMID: 29988846 Free PMC article.
-
Successful intravenous streptokinase therapy in refractory extensive deep vein thrombosis associated with inferior vena cava agenesis: A novel treatment for a rare case.Ann Card Anaesth. 2017 Apr-Jun;20(2):268-269. doi: 10.4103/aca.ACA_211_16. Ann Card Anaesth. 2017. PMID: 28393797 Free PMC article. No abstract available.
-
Exceedingly rare incidence of a double inferior vena cava (IVC) with azygos continuation of left IVC.Clin Case Rep. 2024 May 23;12(6):e8981. doi: 10.1002/ccr3.8981. eCollection 2024 Jun. Clin Case Rep. 2024. PMID: 38799539 Free PMC article.
References
-
- Chee YL, Culligan DJ, Watson HG. Inferior vena cava malformation as a risk factor for deep venous thrombosis in the young. British journal of haematology. 2001 Sep;114(4):878–80. - PubMed
-
- Konopka CL, Salame M, Padulla GA, Muradás RR, Batistella JC. Agenesis of inferior vena cava associated with deep venous thrombosis. Jornal Vascular Brasileiro. 2010 2010 Sep;9(3)
-
- Cho BC, Choi HJ, Kang SM, Chang J, Lee SM, Yang DG, et al. Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolism. Yonsei medical journal. 2004 Oct 31;45(5):947–51. - PubMed
-
- Lambert M, Marboeuf P, Midulla M, Trillot N, Beregi JP, Mounier-Vehier C, et al. Inferior vena cava agenesis and deep vein thrombosis: 10 patients and review of the literature. Vascular medicine. 2010 Dec;15(6):451–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical