

Accuracy of free hand pedicle screw installation in the thoracic and lumbar spine by a young surgeon: an analysis of the first consecutive 306 screws using computed tomography
- PMID: 24967036
- PMCID: PMC4068842
- DOI: 10.4184/asj.2014.8.3.237
Accuracy of free hand pedicle screw installation in the thoracic and lumbar spine by a young surgeon: an analysis of the first consecutive 306 screws using computed tomography
Abstract
Study design: A retrospective cross-sectional study.
Purpose: The purpose of this study is to evaluate the accuracy and safety of free-hand pedicle screw insertion performed by a young surgeon.
Overview of literature: Few articles exist regarding the safety of the free-hand technique without inspection by an experienced spine surgeon.
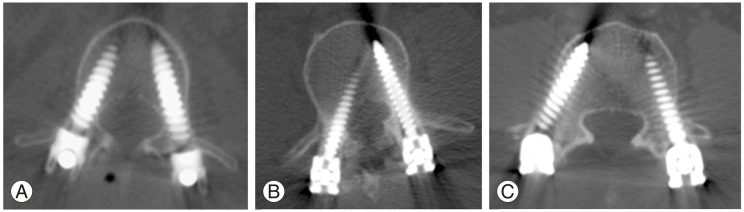
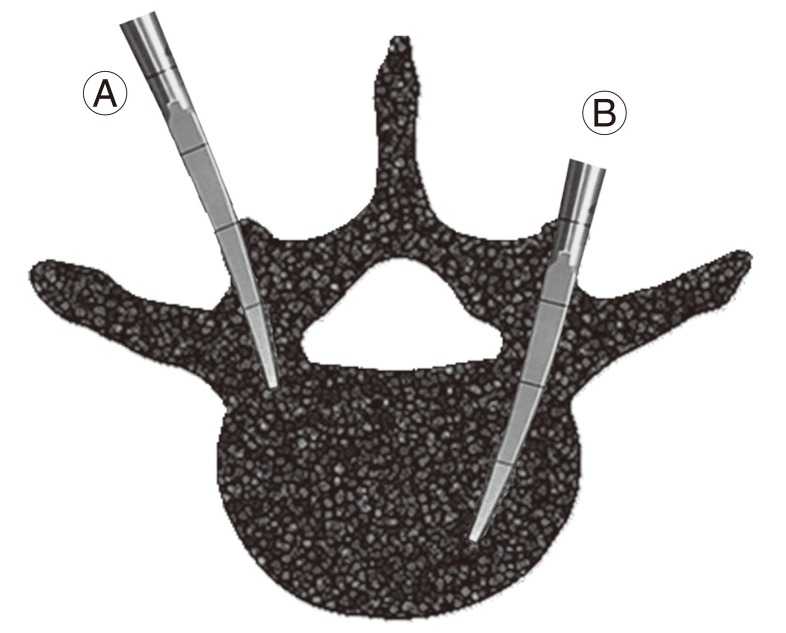
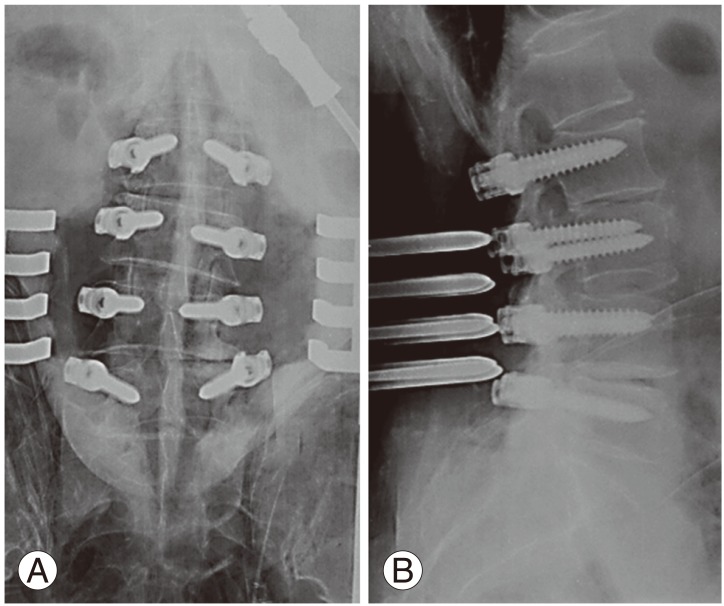
Methods: The index surgeon has performed spinal surgery for 2 years by himself. He performed fluoroscopy-assisted pedicle screw installation for his first year. Since then, he has used the free-hand technique. We retrospectively reviewed the records of all consecutive patients undergoing pedicle screw installation using the free-hand technique without fluoroscopy in the thoracic or lumbar spine by the index surgeon. Incidence and extent of cortical breach by misplaced pedicle screw was determined by a review of postoperative computed tomography (CT) images.
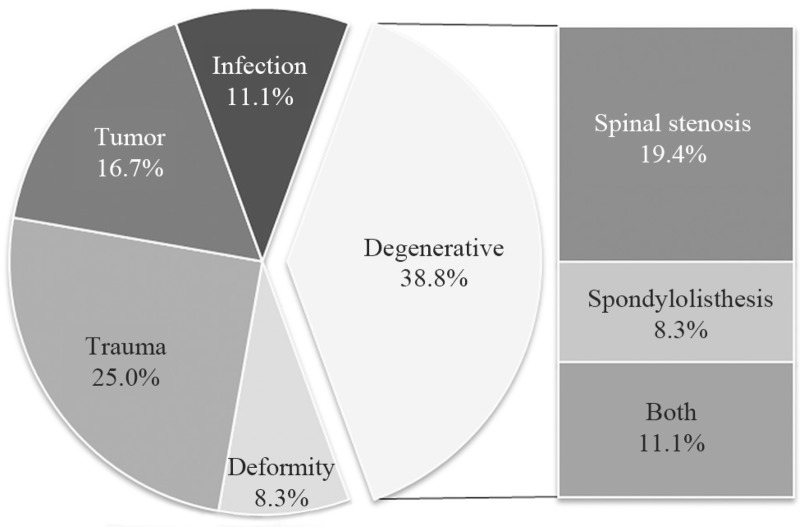
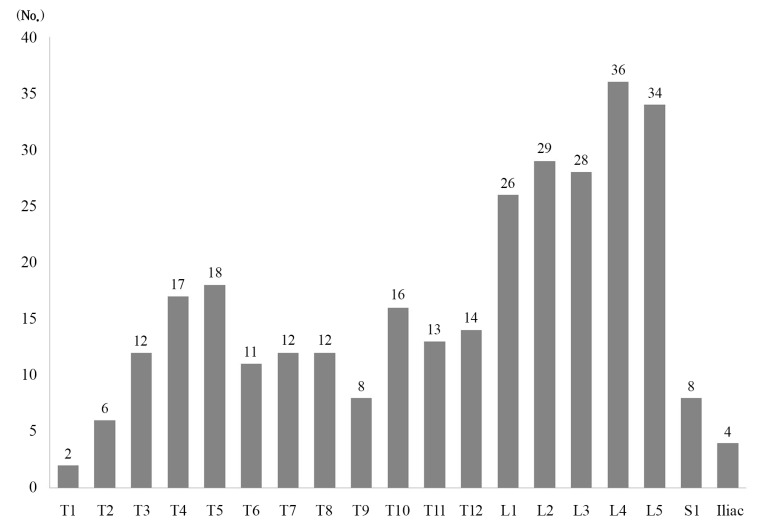
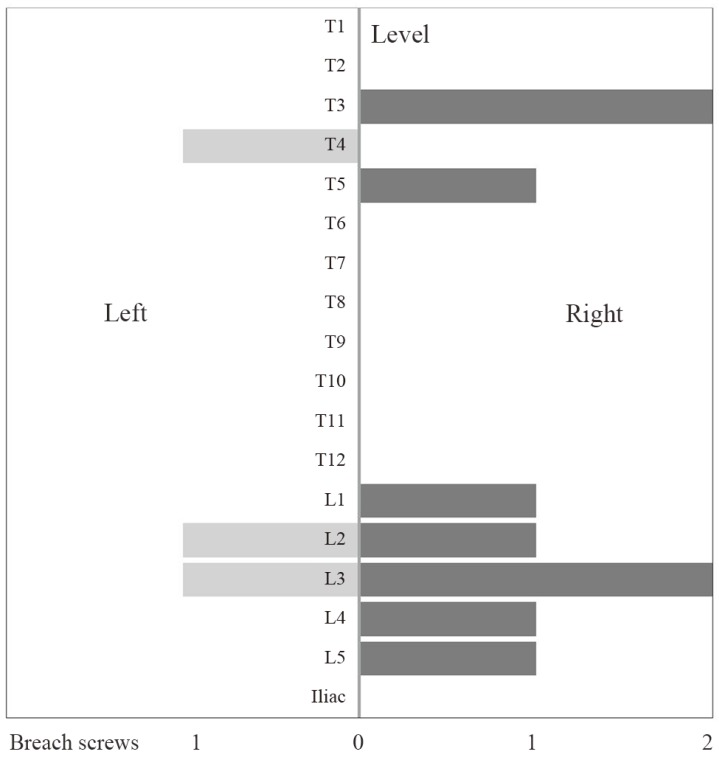
Results: A total of 36 patients received 306 free-hand placed pedicle screws in the thoracic or lumbar spine. A total of 12 screws (3.9%) were identified as breaching the pedicle in 9 patients. Upper thoracic spine was the most frequent location of screw breach (10.8%). Lateral breach (2.3%) was more frequent than any other direction. Screw breach on the right side (9 patients) was more common than that on the left side (3 patients) (p<0.01).
Conclusions: An analysis by CT scan shows that young spine surgeons who have trained under the supervision of an experienced surgeon can safely place free-hand pedicle screws with an acceptable breach rate through repetitive confirmatory steps.
Keywords: Accuracy; Lumbar: Free hand; Pedicle screw; Safety; Thoracic.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Accuracy of free-hand placement of thoracic pedicle screws in adolescent idiopathic scoliosis: how much of a difference does surgeon experience make?Eur Spine J. 2010 Jan;19(1):91-5. doi: 10.1007/s00586-009-1183-6. Epub 2009 Oct 29. Eur Spine J. 2010. PMID: 19882179 Free PMC article.
-
Retrospective computed tomography scan analysis of percutaneously inserted pedicle screws for posterior transpedicular stabilization of the thoracic and lumbar spine: accuracy and complication rates.Spine (Phila Pa 1976). 2012 May 20;37(12):1092-100. doi: 10.1097/BRS.0b013e31823c80d8. Spine (Phila Pa 1976). 2012. PMID: 22037528
-
Accuracy of fluoroscopically-assisted pedicle screw placement: analysis of 1,218 screws in 198 patients.Spine J. 2014 Aug 1;14(8):1702-8. doi: 10.1016/j.spinee.2014.03.044. Epub 2014 Apr 4. Spine J. 2014. PMID: 24704680
-
Breach Rate Analysis of Pedicle Screw Instrumentation using Free-Hand Technique in the Surgical Correction of Adolescent Idiopathic Scoliosis.J Orthop Case Rep. 2021;11(1):38-44. doi: 10.13107/jocr.2021.v11.i01.1956. J Orthop Case Rep. 2021. PMID: 34141640 Free PMC article.
-
Hand-Book for the Military Surgeon.N Am Medchir Rev. 1861 Sep;5(5):818-823. N Am Medchir Rev. 1861. PMID: 38080074 Free PMC article. Review. No abstract available.
Cited by
-
Use of a life-size three-dimensional-printed spine model for pedicle screw instrumentation training.J Orthop Surg Res. 2018 Apr 16;13(1):86. doi: 10.1186/s13018-018-0788-z. J Orthop Surg Res. 2018. PMID: 29661210 Free PMC article.
-
Adolescent Idiopathic Scoliosis Treatment by a Korean Neurosurgeon: The Changing Role for Neurosurgeons.J Korean Neurosurg Soc. 2015 Jul;58(1):50-3. doi: 10.3340/jkns.2015.58.1.50. Epub 2015 Jul 31. J Korean Neurosurg Soc. 2015. PMID: 26279813 Free PMC article.
-
A novel system for accurate lumbar spine pedicle screw placement based on three-dimensional computed tomography reconstruction.J Orthop Translat. 2020 Apr 19;23:101-106. doi: 10.1016/j.jot.2020.03.010. eCollection 2020 Jul. J Orthop Translat. 2020. PMID: 32642424 Free PMC article.
-
Pedicle Screw Placement in the Thoracolumbar Spine Using a Novel, Simple, Safe, and Effective Guide-Pin : A Computerized Tomography Analysis.J Korean Neurosurg Soc. 2015 Jul;58(1):9-13. doi: 10.3340/jkns.2015.58.1.9. Epub 2015 Jul 31. J Korean Neurosurg Soc. 2015. PMID: 26279807 Free PMC article.
-
A novel method to evaluate the transverse pedicle angles of the lower lumbar vertebrae using digital radiography.PLoS One. 2024 Jun 13;19(6):e0295196. doi: 10.1371/journal.pone.0295196. eCollection 2024. PLoS One. 2024. PMID: 38870237 Free PMC article.
References
-
- Boucher HH. A method of spinal fusion. J Bone Joint Surg Br. 1959;41:248–259. - PubMed
-
- Choi WW, Green BA, Levi AD. Computer-assisted fluoroscopic targeting system for pedicle screw insertion. Neurosurgery. 2000;47:872–878. - PubMed
-
- Amiot LP, Lang K, Putzier M, Zippel H, Labelle H. Comparative results between conventional and computer-assisted pedicle screw installation in the thoracic, lumbar, and sacral spine. Spine (Phila Pa 1976) 2000;25:606–614. - PubMed
-
- Youkilis AS, Quint DJ, McGillicuddy JE, Papadopoulos SM. Stereotactic navigation for placement of pedicle screws in the thoracic spine. Neurosurgery. 2001;48:771–778. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
