

Microvascular Endothelial Dysfunction and Enhanced Thromboxane and Endothelial Contractility in Patients with HIV
- PMID: 24967147
- PMCID: PMC4066983
- DOI: 10.4172/2155-6113.1000267
Microvascular Endothelial Dysfunction and Enhanced Thromboxane and Endothelial Contractility in Patients with HIV
Abstract
11 background: The prevalence of cardiovascular disease is increased with human immunodeficiency virus (HIV) infection, but the mechanism is unclear. We hypothesized that HIV increases microvascular reactive oxygen species, thereby impairing endothelial function and enhancing contractility.
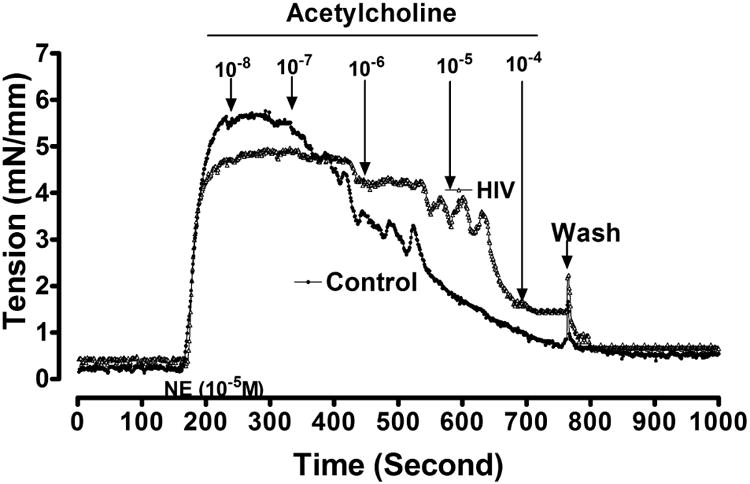
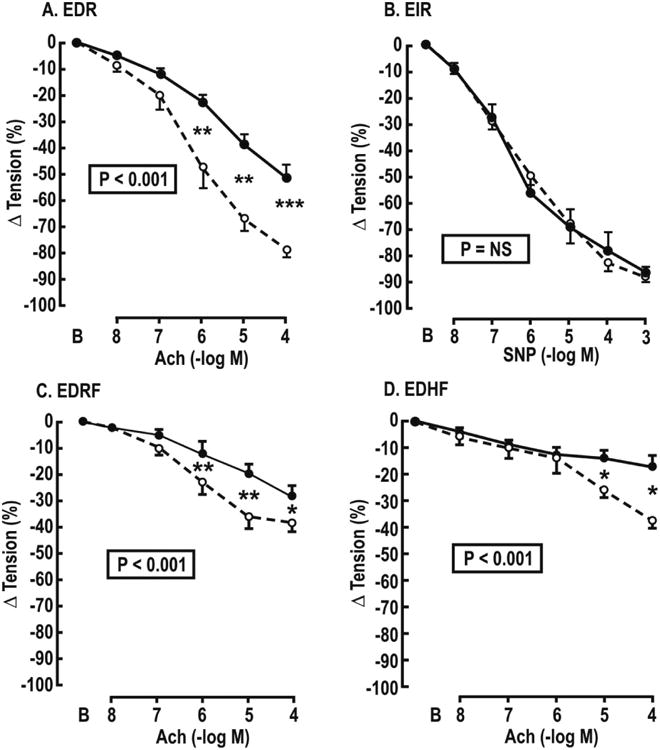
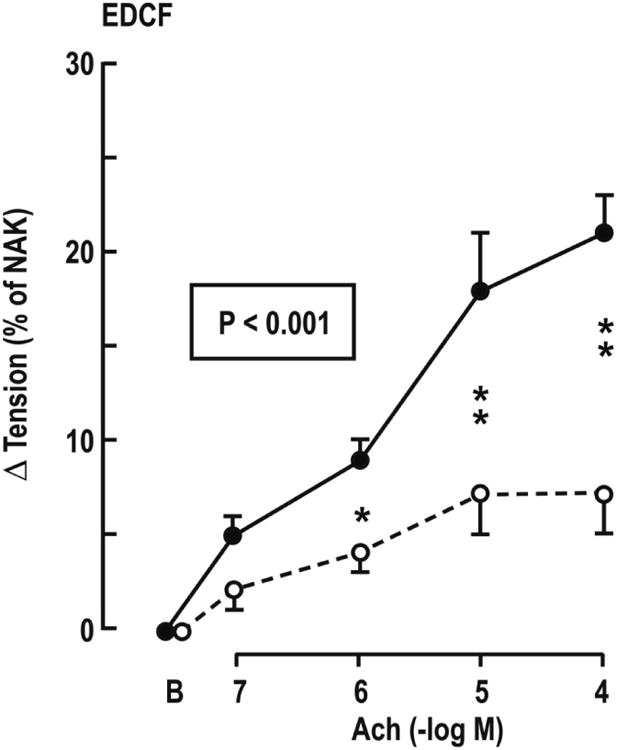
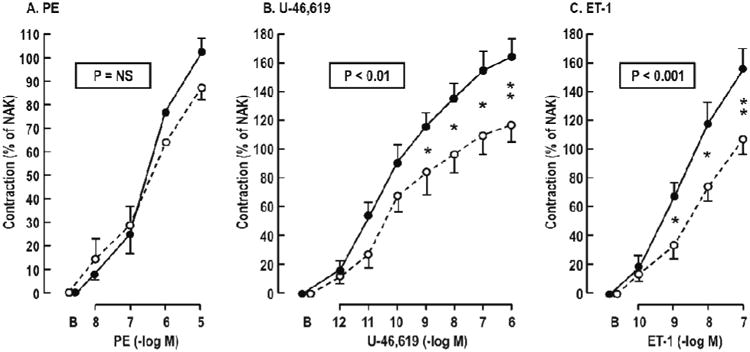
12 method: Subcutaneous microarterioles were isolated from gluteal skin biopsies in premenopausal, African American, HIV positive women receiving effective anti-retroviral therapy, but without cardiovascular risk factors except for increased body mass index (n=10) and healthy matched controls (n=10). The arterioles were mounted on myographs, preconstricted and relaxed with acetylcholine for: endothelium-dependent relaxation, endothelium-dependent relaxation factor (nitric oxide synthase-dependent relaxation), endothelium-dependent hyperpolarizing factor (potassium-channel dependent relaxation) and endothelium-independent relaxation (nitroprusside). Contractions were tested to endothelium-dependent contracting factor (acetylcholine contraction with blocked relaxation); phenylephrine, U-46,619 and endothelin-1. Plasma L-arginine and asymmetric dimethylarginine were measured by high performance capillary electrophoresis.
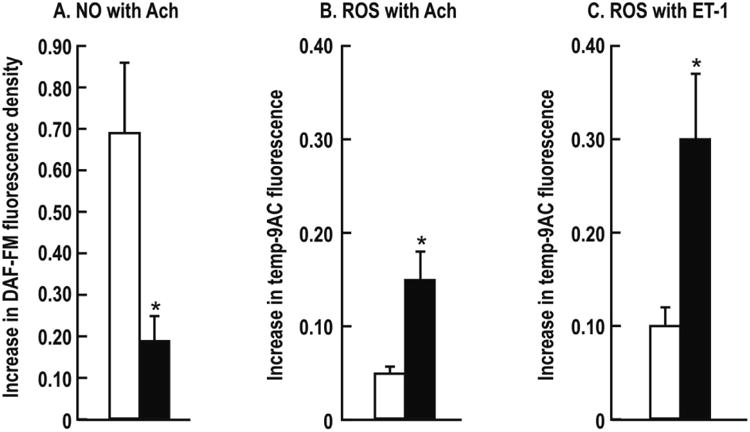
13 results: The micro-arterioles from HIV positive women had significantly (% change in tension; P<0.05) reduced acetylcholine relaxation (-51 ± 6 vs. -78 ± 3%), endothelium-dependent relaxation factor (-28 ± 4 vs. -39 ± 3%), endothelium-dependent hyperpolarizing factor (-17 ± 4 vs. -37 ± 4%) and decreased nitric oxide activity (0.16 ± 0.03 vs. 0.70 ± 0.16 Δ unit) but unchanged nitroprusside relaxation. They had significantly enhanced endothelium-dependent contracting factor (+21 ± 6 vs. +7 ± 2%) and contractions to U-46,619 (+164 ± 10 vs. +117 ± 11%) and endothelin-1(+151 ± 12 vs. +97 ± 9%), but not to phenylephrine. There was enhanced reactive oxygen species with acetylcholine (0.11 ± 0.02 vs. 0.05 ± 0.01 Δ unit; P<0.05) and endothelin-1 (0.31 ± 0.06 vs. 0.10 ± 0.02 Δ unit; P<0.05). Plasma L-arginine: assymetric dimethyl arginine rates was reduced (173 ± 12 vs. 231 ± 6 μmol·μmol-1, P<0.05).
14 conclusion: Premenopausal HIV positive womenhad microvascular oxidative stress with severe endothelial dysfunction and reduced nitric oxide and arginine: assymetric dimethylarginine ratio but enhanced endothelial, thromboxane and endothelin contractions. These microvascular changes may herald later cardiovascular disease.
Keywords: Asymmetric dimethylarginine (ADMA); Cardiovascuar disease (CVD); Endothelial dysfunction; Endothelin-1 (ET-1); Endothelium-dependent relaxing factor (EDRF); Nitric oxide (NO); Reactive oxygen species (ROS); Thromboxane-prostanoid receptors (TP-Rs).
Figures
References
-
- Bozzette SA, Ake CF, Tam HK, Chang SW, Louis TA. Cardiovascular and cerebrovascular events in patients treated for human immunodeficiency virus infection. N Engl J Med. 2003;348:702–710. - PubMed
-
- Hulten E, Mitchell J, Scally J, Gibbs B, Villines TC. HIV positivity, protease inhibitor exposure and subclinical atherosclerosis: a systematic review and meta-analysis of observational studies. Heart. 2009;95:1826–1835. - PubMed
-
- DAD Study Group. Friis-Møller N, Reiss P, Sabin CA, Weber R, et al. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med. 2007;356:1723–1735. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous