

doi: 10.3978/j.issn.2225-319X.2014.05.15.
Natural history of Type B aortic dissection: ten tips
Affiliations
- PMID: 24967163
- PMCID: PMC4052410
- DOI: 10.3978/j.issn.2225-319X.2014.05.15
Item in Clipboard
Natural history of Type B aortic dissection: ten tips
Ann Cardiothorac Surg.
2014 May.
Abstract
We present ten important specific tips regarding the natural history of Type B aortic dissection, which have a bearing on diagnosis and management decisions.
Keywords: Descending thoracic aorta; aortic dissection; indications for surgery; natural history.
Figures
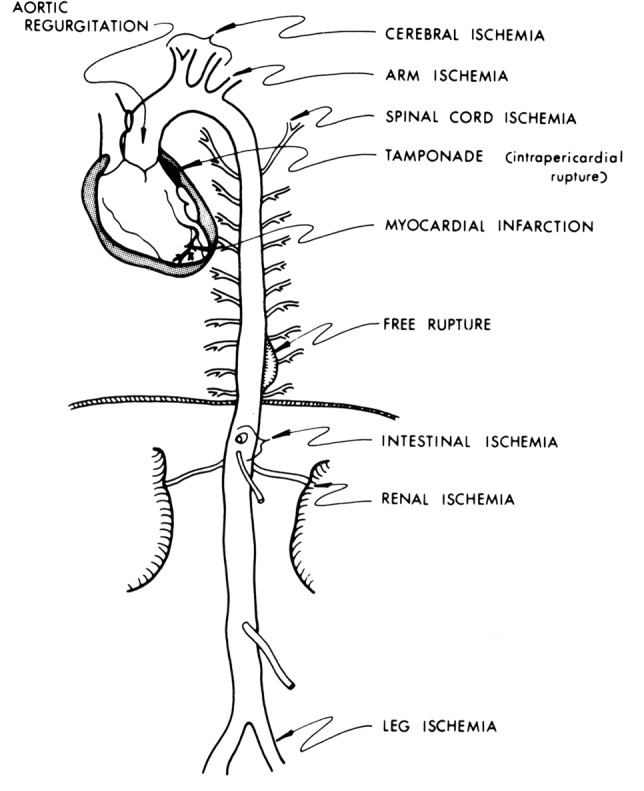
Schematic representation of various conditions that aortic dissection can mimic. [Reprinted with permission from Elefteriades JA. Thoracic aortic aneurysm: reading the enemy’s playbook. Curr Probl Cardiol 2008;33:203-77 (5)].
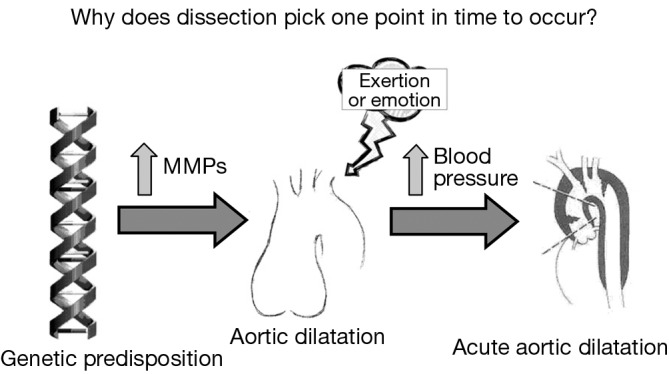
Schematic presentation of possible relationships underlying the instigation of an acute aortic dissection at one particular time. Matrix metalloproteinases [Reprinted with permission from Elefteriades JA. Timing of Acute Aortic Events: How Does Dissection Pick a Date, Time, and Moment to Occur? In: Elefteriades JA. eds. Acute Aortic Disease. New York, NY: Informa Healthcare USA, 2007:169-72. (12)].
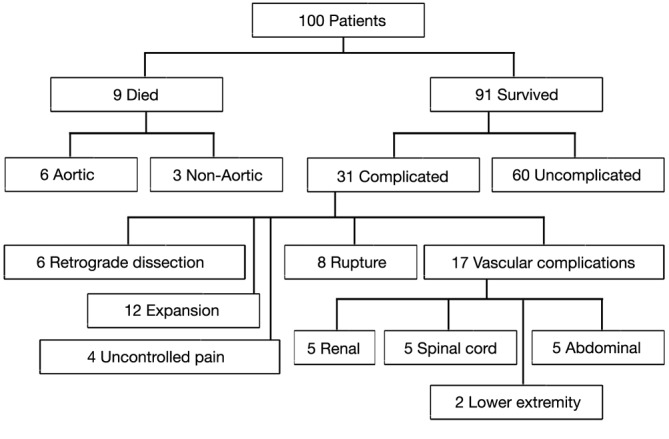
Flow diagram of outcome of 100 consecutive patients with acute descending aortic dissection. [A single patient may have more than one complication.) (Reproduced with permission from Elefteriades JA, Lovoulos CJ, Coady MA, Tellides G, Kopf GS, Rizzo JA. Management of descending aortic dissection. Ann Thorac Surg 1999;67:2002-5. (3)].
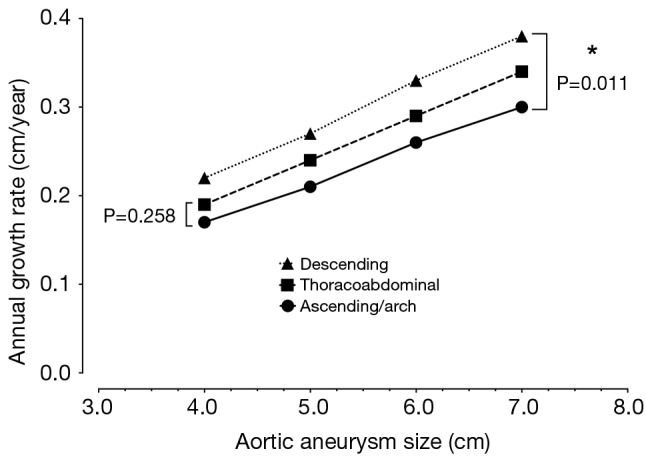
Rates of annual growth of the thoracic aorta.
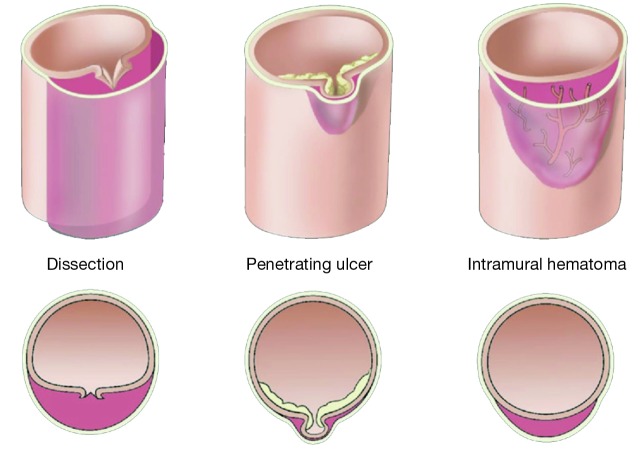
Variant forms of aortic dissection: typical dissection, penetrating aortic ulcer, and intramural hematoma of the aorta. [Reprinted with permission from Elefteriades JA. Thoracic aortic aneurysm: Reading the enemy’s playbook. Curr Probl Cardiol 2008;33:203-77. (5)].
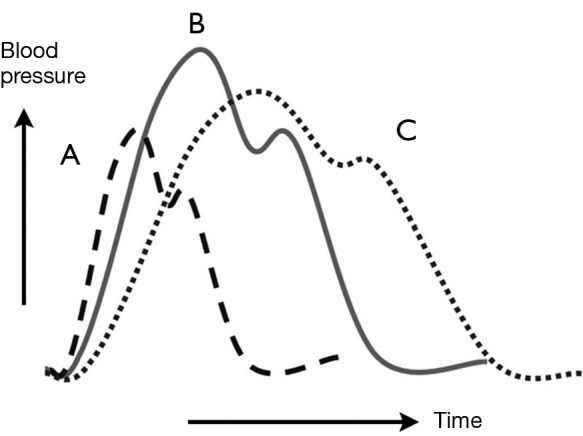
Pharmacologic anti-impulse therapy. Diagram of aortic pressure curves under various conditions. The continuous line (B) represents the baseline state. Administration of a vasodilator agent such as nitroprusside is represented by the dashed curve (A). Beta-blockade administration is represented by the dotted line (C). [Reprinted with permission from Sanz J, Einstein AJ, Fuster V. Acute aortic dissection: Anti-impulse therapy. In: Elefteriades JA. eds. Acute Aortic Disease New York, NY: Informa Healthcare USA, 2007:229-49. (27)].
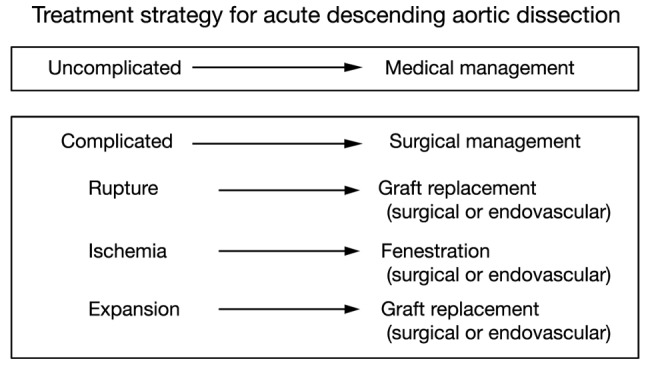
The “complication-specific” approach to acute descending aortic dissection. [Reprinted with permission from Elefteriades JA, Lovoulos CJ, Coady MA, Tellides G, Kopf GS, Rizzo JA. Management of descending aortic dissection. Ann Thorac Surg 1999;67:2002-5; discussion 2014-9. (3)].
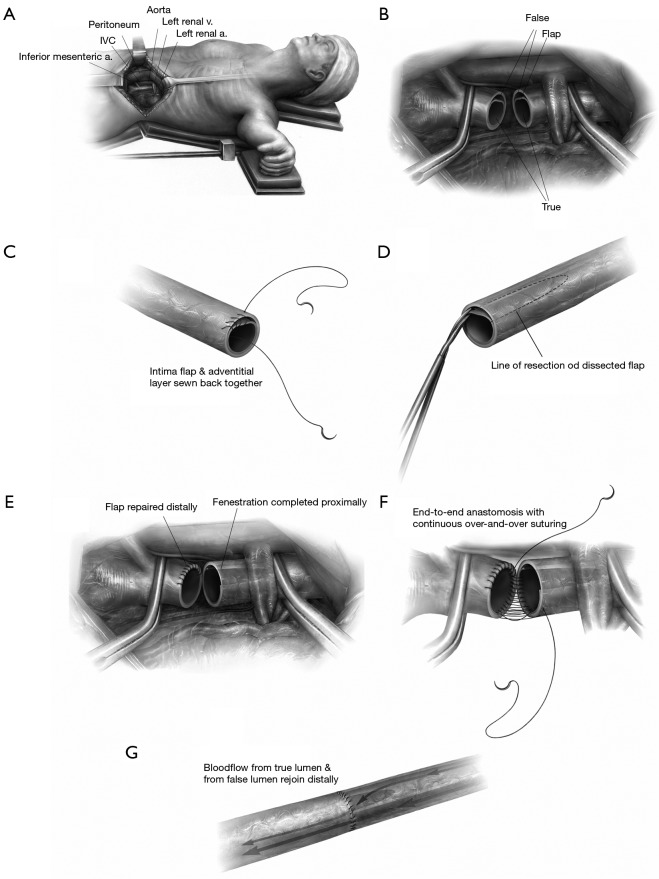
Schematic illustration of the surgical fenestration technique: (A) positioning of the patient, incision, exposure of the retroperitoneal space; (B) the abdominal aorta is clamped proximally and distally, and transected, the dissection flap is visualized; (C) dissection in the distal open end of the aorta is repaired by re-approximate the intima to the adventitial layer; (D) fenestration of the intimal flap is performed on the proximal aorta by excising as much intima as possible, in both circumferential and longitudinal extent toward the proximal clamp; (E,F) the fenestrated proximal end is re-anastamosed to the repaired distal end of the aorta; (G) the clamps are removed and blood flow is restored. [Reprinted with permission from Elefteriades JA, Escalon JC. Aortic Fenestration for Dissection. Operative Techniques in Thoracic and Cardiovascular Surgery 2009;14:12-22. (31)]
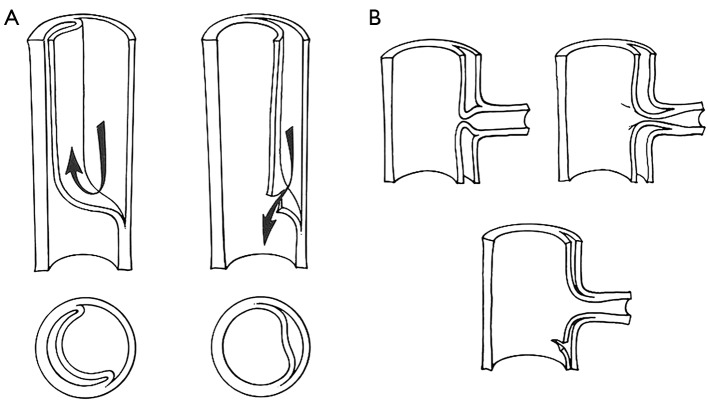
Schematic illustration of the benefit of decompressing the false lumen: (A) schematic diagram of aortic dissection, false lumen formation and decompression of the false lumen; (B) decompression of the false lumen restores blood flow to compromised organs. [Reprinted with permission from Crawford ES, Crawford JL, Smith PS. Diseases of the aorta. Baltimore: Williams & Wilkins, 1984. (32)].
Natural history of Type B aortic dissection: ten tips.
References
-
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 2000;283:897-903 - PubMed
-
- Gallo A, Davies RR, Coe MP, et al. Indications, timing, and prognosis of operative repair of aortic dissections. Semin Thorac Cardiovasc Surg 2005;17:224-35 - PubMed
-
- Elefteriades JA, Lovoulos CJ, Coady MA, et al. Management of descending aortic dissection. Ann Thorac Surg 1999;67:2002-5; discussion 2014-9. - PubMed
-
- Elefteriades JA. Thoracic aortic aneurysm: reading the enemy’s playbook. Current problems in cardiology 2008;33:203-77 - PubMed
LinkOut - more resources
Full Text Sources