

The Navigation Guide - evidence-based medicine meets environmental health: systematic review of human evidence for PFOA effects on fetal growth
- PMID: 24968388
- PMCID: PMC4181929
- DOI: 10.1289/ehp.1307893
The Navigation Guide - evidence-based medicine meets environmental health: systematic review of human evidence for PFOA effects on fetal growth
Abstract
Background: The Navigation Guide methodology was developed to meet the need for a robust method of systematic and transparent research synthesis in environmental health science. We conducted a case study systematic review to support proof of concept of the method.
Objective: We applied the Navigation Guide systematic review methodology to determine whether developmental exposure to perfluorooctanoic acid (PFOA) affects fetal growth in humans.
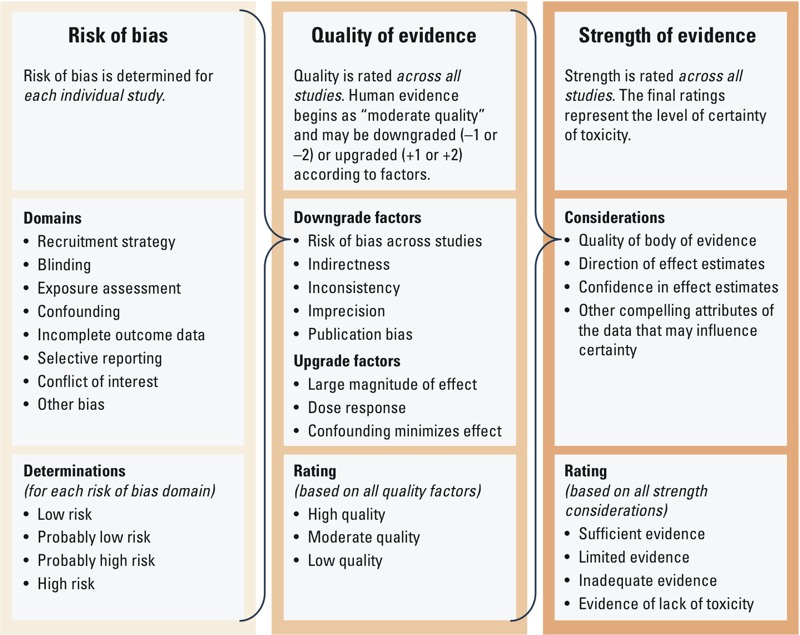
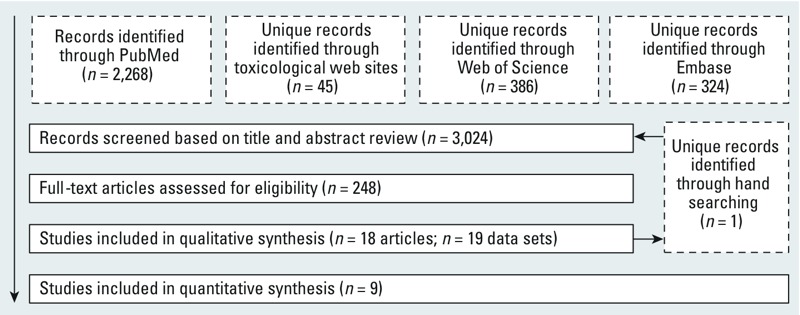
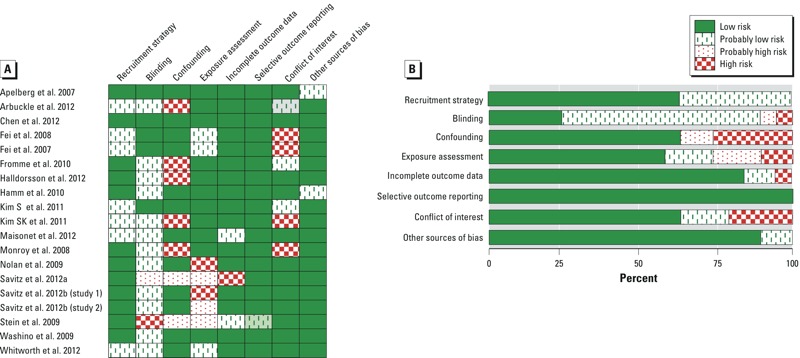
Methods: We applied the first 3 steps of the Navigation Guide methodology to human epidemiological data: 1) specify the study question, 2) select the evidence, and 3) rate the quality and strength of the evidence. We developed a protocol, conducted a comprehensive search of the literature, and identified relevant studies using prespecified criteria. We evaluated each study for risk of bias and conducted meta-analyses on a subset of studies. We rated quality and strength of the entire body of human evidence.
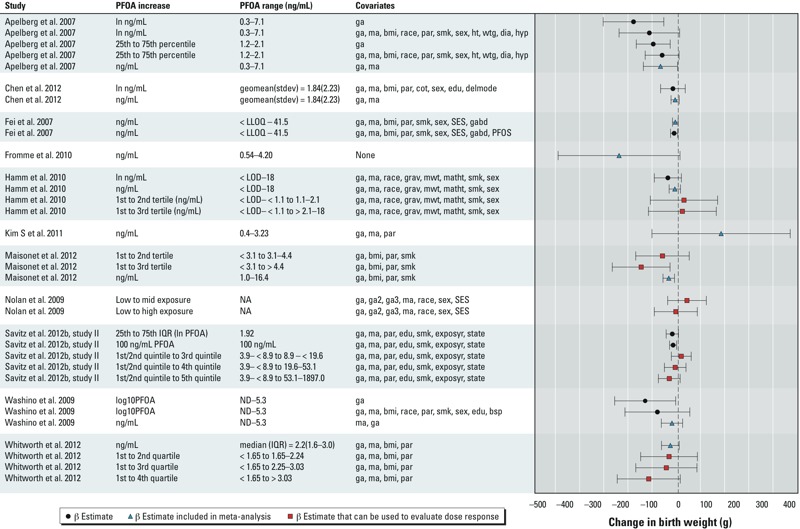
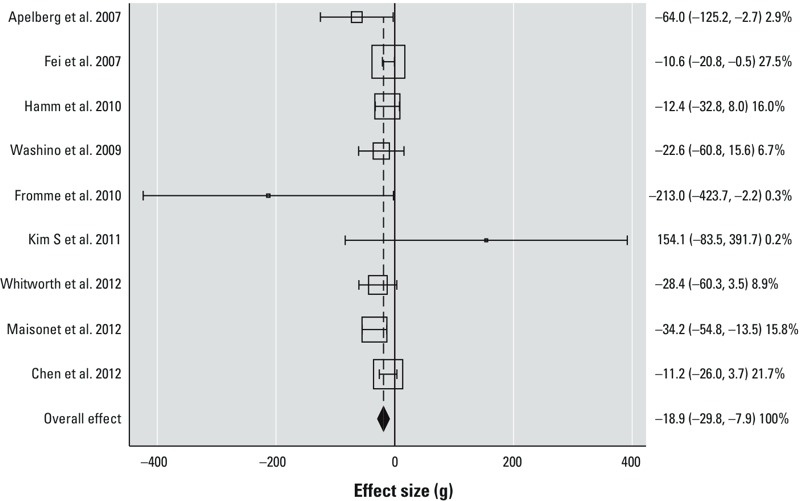
Results: We identified 18 human studies that met our inclusion criteria, and 9 of these were combined through meta-analysis. Through meta-analysis, we estimated that a 1-ng/mL increase in serum or plasma PFOA was associated with a -18.9 g (95% CI: -29.8, -7.9) difference in birth weight. We concluded that the risk of bias across studies was low, and we assigned a "moderate" quality rating to the overall body of human evidence.
Conclusion: On the basis of this first application of the Navigation Guide systematic review methodology, we concluded that there is "sufficient" human evidence that developmental exposure to PFOA reduces fetal growth.
Conflict of interest statement
The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the U.S. EPA. Further, the U.S. EPA does not endorse the purchase of any commercial products or services mentioned in the publication.
The authors declare they have no actual or potential competing financial interests.
Figures
Comment in
-
The Navigation Guide: systematic review for the environmental health sciences.Environ Health Perspect. 2014 Oct;122(10):A283. doi: 10.1289/ehp.122-A283. Environ Health Perspect. 2014. PMID: 25271710 Free PMC article. No abstract available.
-
Systematic reviews: perhaps "the answer to policy makers' prayers"?Environ Health Perspect. 2014 Oct;122(10):A262-3. doi: 10.1289/ehp.1408599. Environ Health Perspect. 2014. PMID: 25272205 Free PMC article. No abstract available.
References
-
- Agency for Toxic Substances and Disease Registry. Draft Toxicological Profile for Perfluoroalkyls. Atlanta, GA: Agency for Toxic Substances and Disease Registry. 2009. Available: http://www.atsdr.cdc.gov/toxprofiles/tp200.pdf [accessed 29 August 2014] - PubMed
-
- Arbuckle TE, Kubwabo C, Walker M, Davis K, Lalonde K, Kosarac I, et al. Umbilical cord blood levels of perfluoroalkyl acids and polybrominated flame retardants. Int J Hyg Environ Health. 2012;216:184–194. - PubMed
-
- Azzalini A, Capitanio A. Distributions generated by perturbation of symmetry with emphasis on a multivariate skew t-distribution. J R Stat Soc Series B Stat Methodol. 2003;65:367–389.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
