

Regular examinations for toxic maculopathy in long-term chloroquine or hydroxychloroquine users
- PMID: 24970348
- PMCID: PMC4192095
- DOI: 10.1001/jamaophthalmol.2014.1720
Regular examinations for toxic maculopathy in long-term chloroquine or hydroxychloroquine users
Abstract
Importance: According to evidence-based, expert recommendations, long-term users of chloroquine or hydroxychloroquine sulfate should undergo regular visits to eye care providers and diagnostic testing to check for maculopathy.
Objective: To determine whether patients with rheumatoid arthritis (RA) or systemic lupus erythematosus (SLE) taking chloroquine or hydroxychloroquine are regularly visiting eye care providers and being screened for maculopathy.
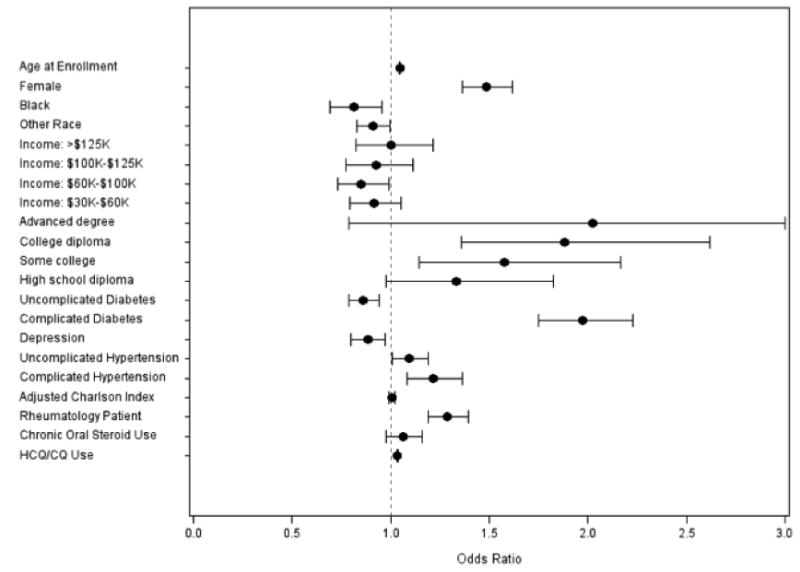
Design, setting, and participants: Patients with RA or SLE who were continuously enrolled in a particular managed care network for at least 5 years between January 1, 2001, and December 31, 2011, were studied. Patients' amount of chloroquine or hydroxychloroquine use in the 5 years since the initial RA or SLE diagnosis was calculated, along with their number of eye care visits and diagnostic tests for maculopathy. Those at high risk for maculopathy were identified. Logistic regression was performed to assess potential factors associated with regular eye care visits (annual visits in ≥3 of 5 years) among chloroquine or hydroxychloroquine users, including those at highest risk for maculopathy.
Main outcomes and measures: Among chloroquine or hydroxychloroquine users and those at high risk for toxic maculopathy, the proportions with regular eye care visits and diagnostic testing, as well as the likelihood of regular eye care visits.
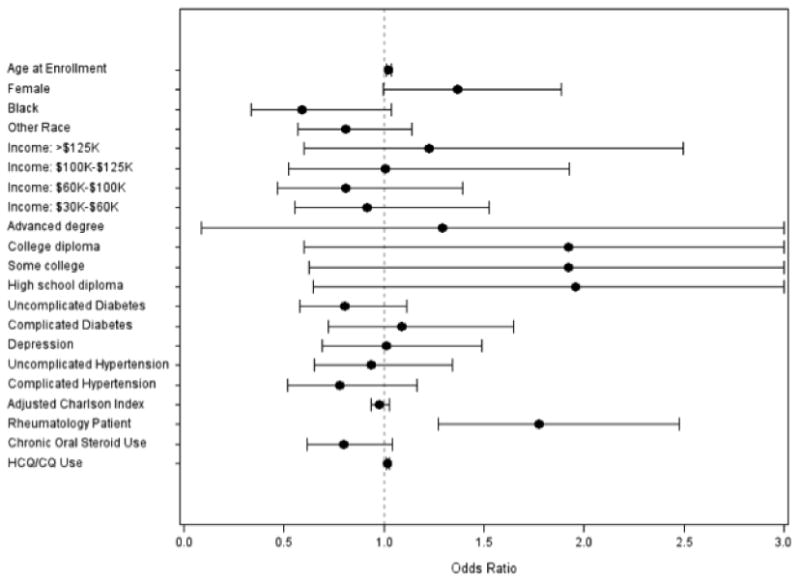
Results: Among 18 051 beneficiaries with RA or SLE, 6339 (35.1%) had at least 1 record of chloroquine or hydroxychloroquine use, and 1409 (7.8%) had used chloroquine or hydroxychloroquine for at least 4 years. Among those at high risk for maculopathy, 27.9% lacked regular eye care visits, 6.1% had no visits to eye care providers, and 34.5% had no diagnostic testing for maculopathy during the 5-year period. Among high-risk patients, each additional month of chloroquine or hydroxychloroquine use was associated with a 2.0% increased likelihood of regular eye care (adjusted odds ratio, 1.02; 95% CI, 1.01-1.03). High-risk patients whose SLE or RA was managed by rheumatologists had a 77.4% increased likelihood of regular eye care (adjusted odds ratio, 1.77; 95% CI, 1.27-2.47) relative to other patients.
Conclusions and relevance: In this insured population, many patients at high risk for maculopathy associated with the use of chloroquine or hydroxychloroquine are not undergoing routine monitoring for this serious adverse effect. Future studies should explore factors contributing to suboptimal adherence to expert guidelines and the potential effect on patients' vision-related outcomes.
Figures
Comment in
-
Hydroxychloroquine and the retina.JAMA. 2015 Feb 24;313(8):847-8. doi: 10.1001/jama.2014.14558. JAMA. 2015. PMID: 25710661 No abstract available.
References
-
- Ruiz-Irastoza G, Ramos-Casais M, Brito-Zeron P, Khamashata MA. Clinical efficacy and side effects of antimalarials in systemic lupus erythematosus: a systematic review. Ann Rheum Dis. 2010;69(1):20–8. - PubMed
-
- O'Dell JR, Haire CE, Erikson N, et al. Treatment of rheumatoid arthritis with methotrexate alone, sulfasalazine and hydroxychloroquine, or a combination of all three medications. N Engl J Med. 1996;334(20):1287–91. - PubMed
-
- Dubois EL. Antimalarials in the management of discoid and systemic lupus erythematosus. Semin Arthritis Rheum. 1978;8(1):33–51. - PubMed
-
- Wallace DJ. The history of antimalarials. Lupus. 1996;5(Suppl 1):S2–S3. - PubMed
-
- Suarez-Almazor ME, Belseck E, Shea B, Homik J, Wells G, Tugwell P. Antimalarials for treating rheumatoid arthritis. Cochrane Database Syst Rev. 2000;(4):CD000959. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
