

Detection of minimal residual disease in B lymphoblastic leukemia by high-throughput sequencing of IGH
- PMID: 24970842
- PMCID: PMC5142743
- DOI: 10.1158/1078-0432.CCR-13-3231
Detection of minimal residual disease in B lymphoblastic leukemia by high-throughput sequencing of IGH
Abstract
Purpose: High-throughput sequencing (HTS) of immunoglobulin heavy-chain genes (IGH) in unselected clinical samples for minimal residual disease (MRD) in B lymphoblastic leukemia (B-ALL) has not been tested. As current MRD-detecting methods such as flow cytometry or patient-specific qPCR are complex or difficult to standardize in the clinical laboratory, sequencing may enhance clinical prognostication.
Experimental design: We sequenced IGH in paired pretreatment and day 29 post-treatment samples using residual material from consecutive, unselected samples from the Children's Oncology Group AALL0932 trial to measure MRD as compared with flow cytometry. We assessed the impact of ongoing recombination at IGH on MRD detection in post-treatment samples. Finally, we evaluated a subset of cases with discordant MRD results between flow cytometry and sequencing.
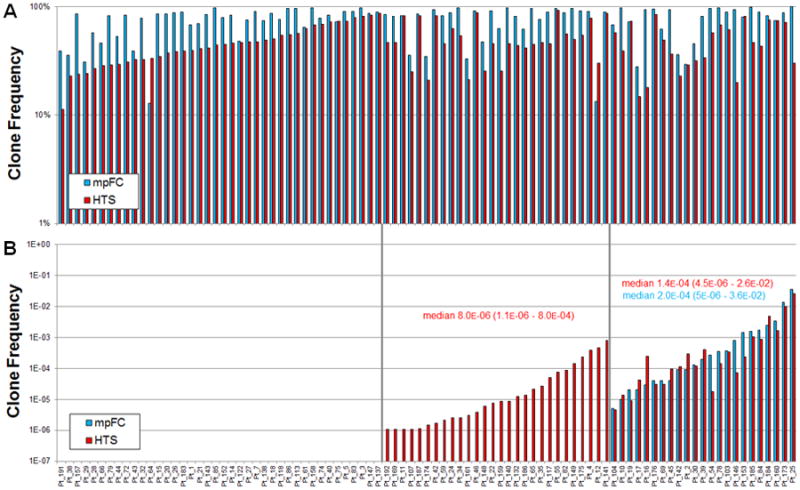
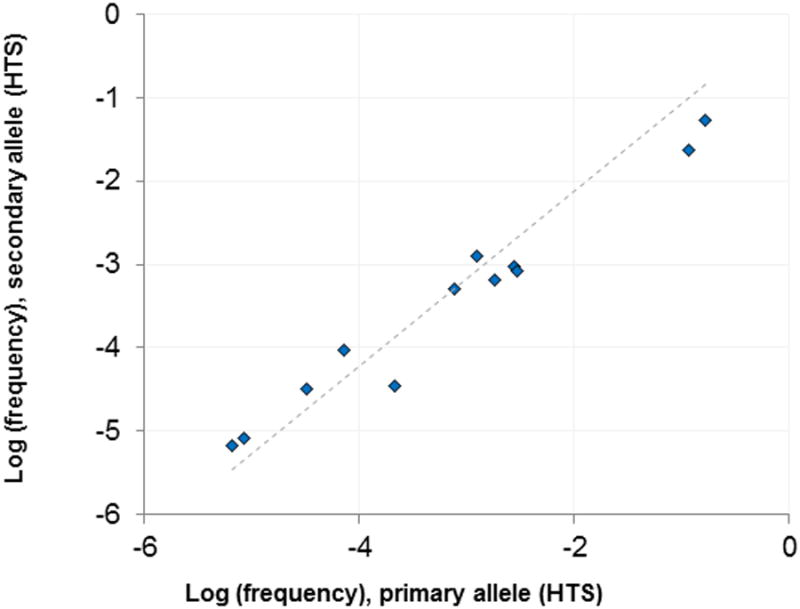
Results: We found clonal IGH rearrangements in 92 of 98 pretreatment patient samples. Furthermore, while ongoing recombination of IGH was evident, index clones typically prevailed in MRD-positive post-treatment samples, suggesting that clonal evolution at IGH does not contribute substantively to tumor fitness. MRD was detected by sequencing in all flow cytometry-positive cases with no false-negative results. In addition, in a subset of patients, MRD was detected by sequencing, but not by flow cytometry, including a fraction with MRD levels within the sensitivity of flow cytometry. We provide data that suggest that this discordance in some patients may be due to the phenotypic maturation of the transformed cell.
Conclusion: Our results provide strong support for HTS of IGH to enhance clinical prognostication in B-ALL.
©2014 American Association for Cancer Research.
Conflict of interest statement
H.R. and C.C. have consultancy, equity ownership, patents & royalties with Adaptive Biotechnologies; R.E, A.S., B.H., J.V., M.R., I.K., C.C. and D.W.W., have employment and equity ownership with Adaptive Biotechnologies; B.W. has research funding from Becton, Dickinson and Company, NJ; D. Wu, B.W., with H.R. and Adaptive Biotechnologies are collaborating on a related research project examining next-generation sequencing for mature B- and T-cell lymphomas. M.L.L. and A.A. have no relevant conflicts of interest to disclose.
Figures
References
-
- Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med. 2006;354:166–78. - PubMed
-
- Bruggemann M, Raff T, Kneba M. Has MRD monitoring superseded other prognostic factors in adult ALL? Blood. 2012;120:4470–81. - PubMed
-
- Campana D. Minimal residual disease in acute lymphoblastic leukemia. Hematology Am Soc Hematol Educ Program. 2010;2010:7–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
