

A randomized multicenter trial of paricalcitol versus calcitriol for secondary hyperparathyroidism in stages 3-4 CKD
- PMID: 24970869
- PMCID: PMC4152818
- DOI: 10.2215/CJN.10661013
A randomized multicenter trial of paricalcitol versus calcitriol for secondary hyperparathyroidism in stages 3-4 CKD
Abstract
Background and objectives: Calcitriol is used to treat secondary hyperparathyroidism in patients with CKD. Paricalcitol is less calcemic and phosphatemic in preclinical studies and in some trials in dialysis patients, but head-to-head comparisons in nondialysis patients are lacking. A large meta-analysis of trials concluded that these agents did not consistently reduce parathyroid hormone (PTH) and increased the risk of hypercalcemia and hyperphosphatemia. Therefore, the objective of this multicenter trial was to compare the rate of hypercalcemia between calcitriol and paricalcitol, while suppressing PTH 40%-60%.
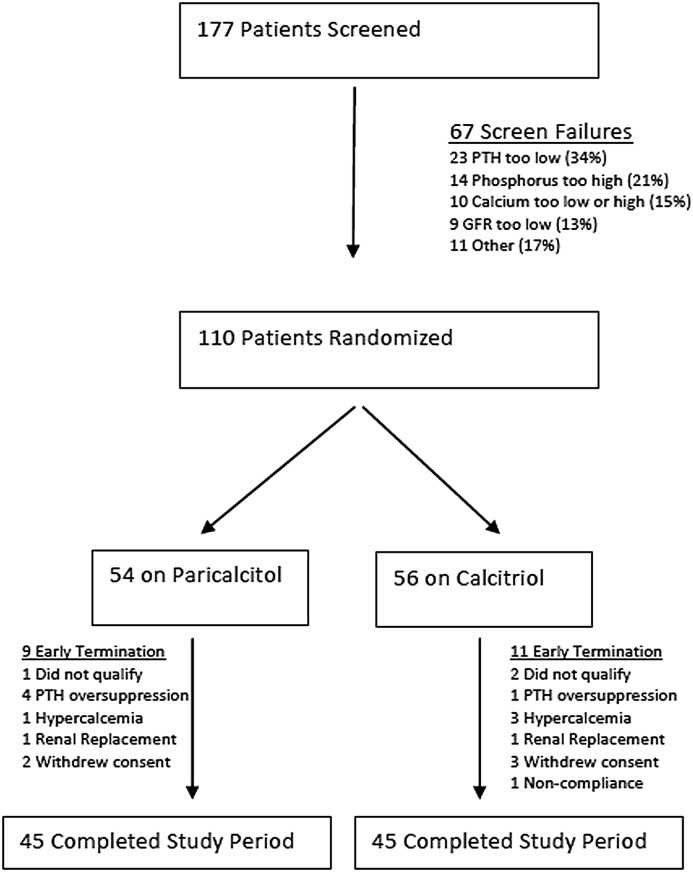
Design, setting, participants, & measurements: Patients with stages 3-4 CKD (n=110) with a PTH level >120 pg/ml were recruited and randomized to 0.25 μg/d of calcitriol or 1 μg/d of paricalcitol between April 2009 and July 2011. Subsequent dose adjustments were by protocol to achieve 40%-60% PTH suppression below baseline. The primary endpoint was the rate of confirmed hypercalcemia of >10.5 mg/dl between groups.
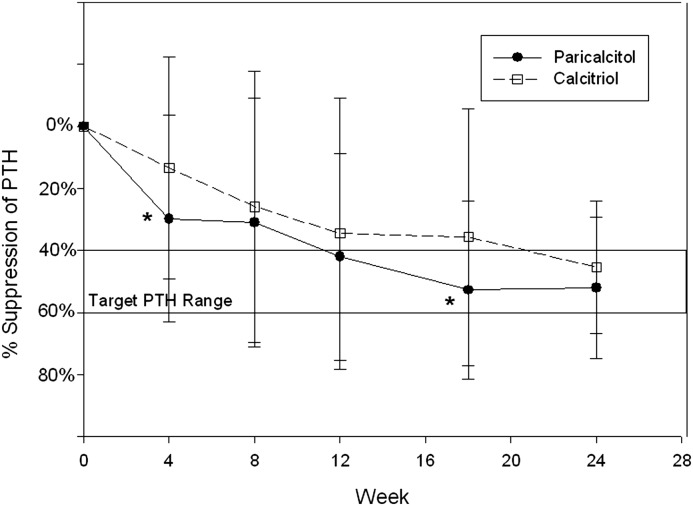
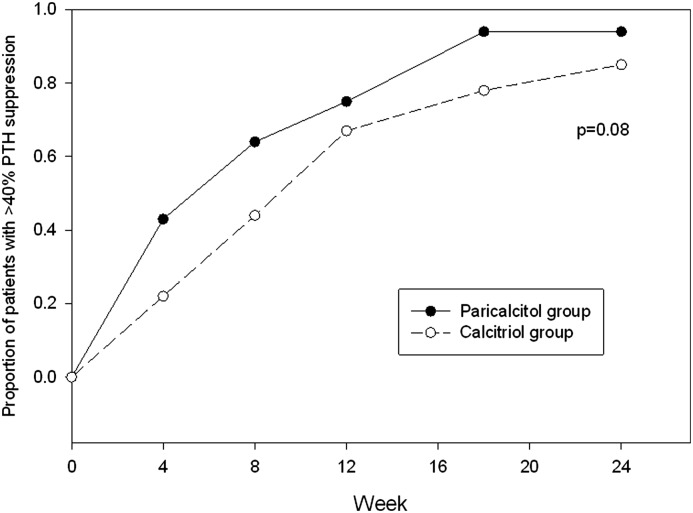
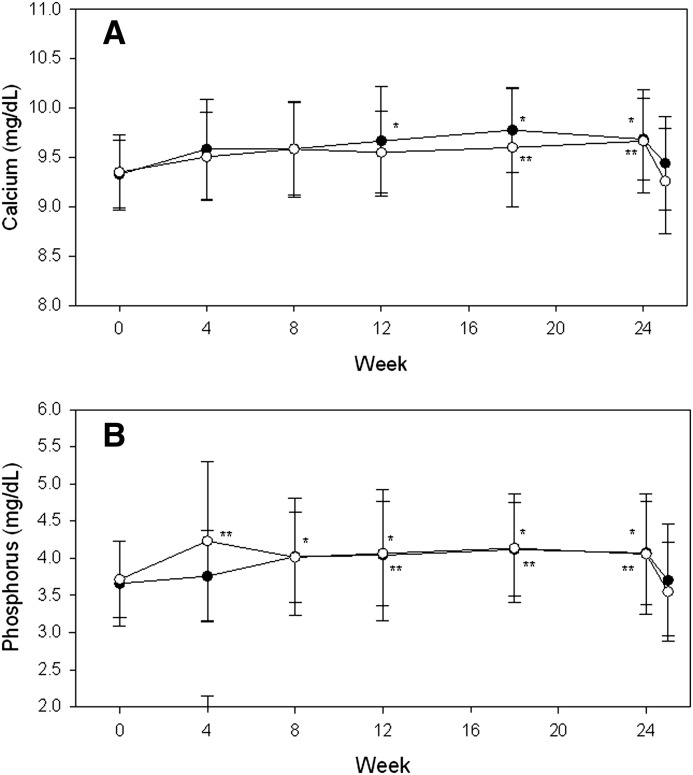
Results: Forty-five patients in each group completed the 24 weeks of treatment. Both agents suppressed PTH effectively (-52% with paricalcitol and -46% with calcitriol; P=0.17), although the paricalcitol group reached a 40% reduction in PTH sooner at a median 8 weeks (interquartile range [IQR], 4, 12) versus 12 weeks (IQR, 8, 18; P=0.02) and had a lower pill burden of 240 (IQR, 180, 298) versus 292 (IQR, 231, 405; P=0.01). Confirmed hypercalcemia was very low in both groups (three with paricalcitol and one with calcitriol) and was not significantly different (P=0.36). Both groups had small increases in calcium and phosphorus levels (0.3-0.4 mg/dl in each electrolyte) and significant decreases in alkaline phosphatase, a marker of high bone turnover, with no significant differences between groups.
Conclusions: These results show that both calcitriol and paricalcitol achieved sustained PTH and alkaline phosphatase suppression in stages 3-4 CKD, with small effects on serum calcium and phosphorus and a low incidence of hypercalcemia.
Keywords: calcium; chronic renal disease; hyperparathyroidism; vitamin D.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL: Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int 71: 31–38, 2007 - PubMed
-
- de Francisco AL: Secondary hyperparathyroidism: Review of the disease and its treatment. Clin Ther 26: 1976–1993, 2004 - PubMed
-
- Sprague SM, Lerma E, McCormmick D, Abraham M, Batlle D: Suppression of parathyroid hormone secretion in hemodialysis patients: Comparison of paricalcitol with calcitriol. Am J Kidney Dis 38[Suppl 5]: S51–S56, 2001 - PubMed
-
- Sprague SM, Llach F, Amdahl M, Taccetta C, Batlle D: Paricalcitol versus calcitriol in the treatment of secondary hyperparathyroidism. Kidney Int 63: 1483–1490, 2003 - PubMed
-
- Ross EA, Tian J, Abboud H, Hippensteel R, Melnick JZ, Pradhan RS, Williams LA, Hamm LL, Sprague SM: Oral paricalcitol for the treatment of secondary hyperparathyroidism in patients on hemodialysis or peritoneal dialysis. Am J Nephrol 28: 97–106, 2008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
