

Current status of granulocyte-macrophage colony-stimulating factor in the immunotherapy of melanoma
- PMID: 24971166
- PMCID: PMC4072479
- DOI: 10.1186/2051-1426-2-11
Current status of granulocyte-macrophage colony-stimulating factor in the immunotherapy of melanoma
Abstract
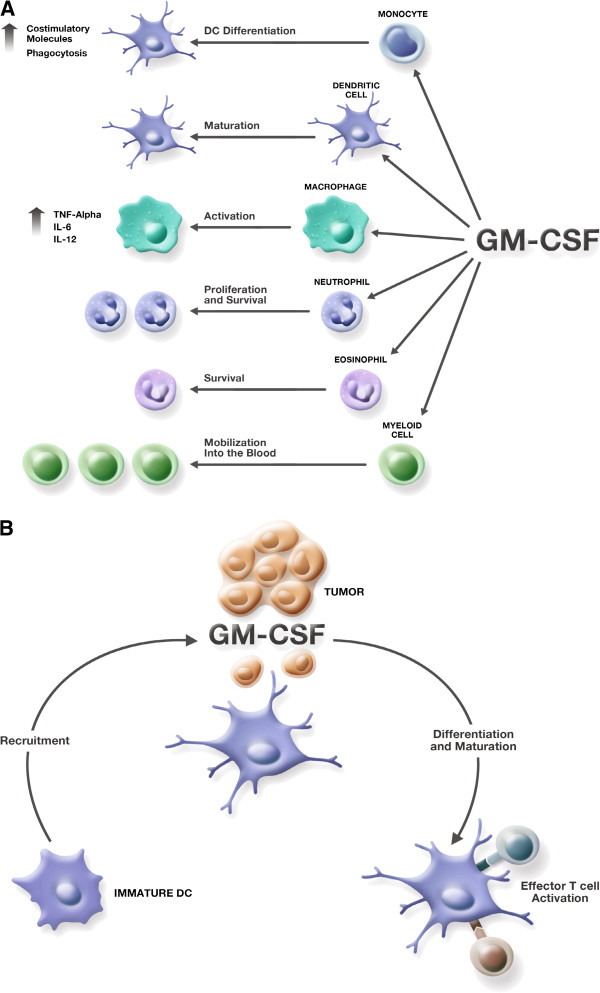
In 2012, it was estimated that 9180 people in the United States would die from melanoma and that more than 76,000 new cases would be diagnosed. Surgical resection is effective for early-stage melanoma, but outcomes are poor for patients with advanced disease. Expression of tumor-associated antigens by melanoma cells makes the disease a promising candidate for immunotherapy. The hematopoietic cytokine granulocyte-macrophage colony-stimulating factor (GM-CSF) has a variety of effects on the immune system including activation of T cells and maturation of dendritic cells, as well as an ability to promote humoral and cell-mediated responses. Given its immunobiology, there has been interest in strategies incorporating GM-CSF in the treatment of melanoma. Preclinical studies with GM-CSF have suggested that it has antitumor activity against melanoma and can enhance the activity of anti-melanoma vaccines. Numerous clinical studies have evaluated recombinant GM-CSF as a monotherapy, as adjuvant with or without cancer vaccines, or in combination with chemotherapy. Although there have been suggestions of clinical benefit in some studies, results have been inconsistent. More recently, novel approaches incorporating GM-CSF in the treatment of melanoma have been evaluated. These have included oncolytic immunotherapy with the GM-CSF-expressing engineered herpes simplex virus talimogene laherparepvec and administration of GM-CSF in combination with ipilimumab, both of which have improved patient outcomes in phase 3 studies. This review describes the diverse body of preclinical and clinical evidence regarding use of GM-CSF in the treatment of melanoma.
Keywords: Cellular immunotherapy; GM-CSF; Granulocyte macrophage-colony stimulating factor; Melanoma.
Figures
References
-
- National Comprehensive Cancer Network. NCCN Guidelines® Version 2.2013 Melanoma. Fort Washington, PA; 2012.
-
- Eggermont AM, Suciu S, Santinami M, Testori A, Kruit WH, Marsden J, Punt CJ, Sales F, Gore M, Mackie R, Kusic Z, Dummer R, Hauschild A, Musat E, Spatz A, Keilholz U, Group EM. Adjuvant therapy with pegylated interferon alfa-2b versus observation alone in resected stage III melanoma: final results of EORTC 18991, a randomised phase III trial. Lancet. 2008;372:117–126. doi: 10.1016/S0140-6736(08)61033-8. - DOI - PubMed
-
- Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbe C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. doi: 10.1056/NEJMoa1003466. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources