

Surgical technique in distal pancreatectomy: a systematic review of randomized trials
- PMID: 24971333
- PMCID: PMC4058114
- DOI: 10.1155/2014/482906
Surgical technique in distal pancreatectomy: a systematic review of randomized trials
Abstract
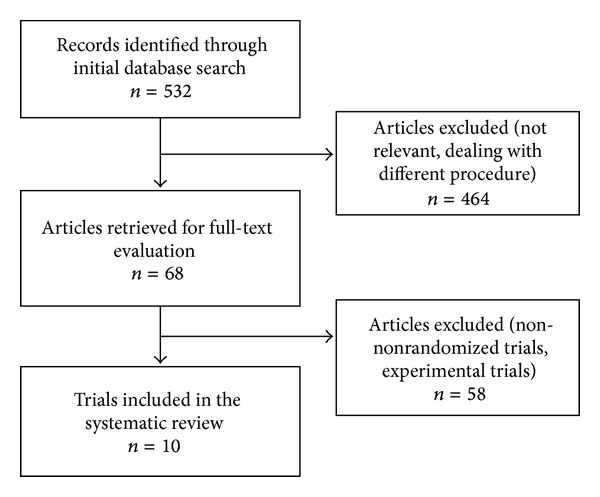
Despite recent improvements in surgical technique, the morbidity of distal pancreatectomy remains high, with pancreatic fistula being the most significant postoperative complication. A systematic review of randomized controlled trials (RCTs) dealing with surgical techniques in distal pancreatectomy was carried out to summarize up-to-date knowledge on this topic. The Cochrane Central Registry of Controlled Trials, Embase, Web of Science, and Pubmed were searched for relevant articles published from 1990 to December 2013. Ten RCTs were identified and included in the systematic review, with a total of 1286 patients being randomized (samples ranging from 41 to 450). The reviewers were in agreement for application of the eligibility criteria for study selection. It was not possible to carry out meta-analysis of these studies because of the heterogeneity of surgical techniques and approaches, such as varying methods of pancreas transection, reinforcement of the stump with seromuscular patch or pancreaticoenteric anastomosis, sealing with fibrin sealants and pancreatic stent placement. Management of the pancreatic remnant after distal pancreatectomy is still a matter of debate. The results of this systematic review are possibly biased by methodological problems in some of the included studies. New well designed and carefully conducted RCTs must be performed to establish the optimal strategy for pancreatic remnant management after distal pancreatectomy.
Figures
References
-
- Büchler MW, Wagner M, Schmied BM, et al. Changes in morbidity after pancreatic resection: toward the end of completion pancreatectomy. Archives of Surgery. 2003;138(12):1310–1314. - PubMed
-
- Nathan H, Cameron JL, Goodwin CR, et al. Risk factors for pancreatic leak after distal pancreatectomy. Annals of Surgery. 2009;250(2):277–281. - PubMed
-
- Pratt W, Maithel SK, Vanounou T, Callery MP, Vollmer CM., Jr. Postoperative pancreatic fistulas are not equivalent after proximal, distal, and central pancreatectomy. Journal of Gastrointestinal Surgery. 2006;10(9):1264–1279. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
