

Primary vs. secondary antibody deficiency: clinical features and infection outcomes of immunoglobulin replacement
- PMID: 24971644
- PMCID: PMC4074074
- DOI: 10.1371/journal.pone.0100324
Primary vs. secondary antibody deficiency: clinical features and infection outcomes of immunoglobulin replacement
Abstract
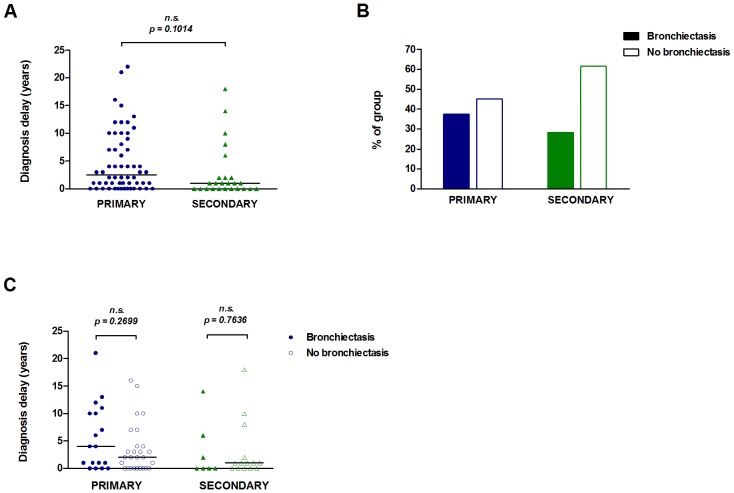
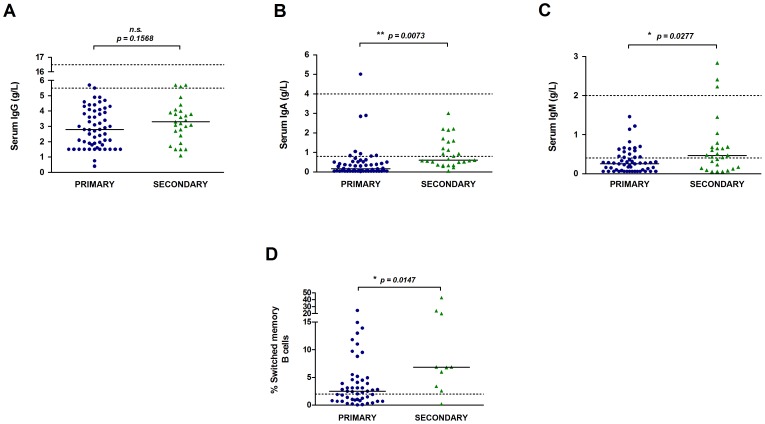
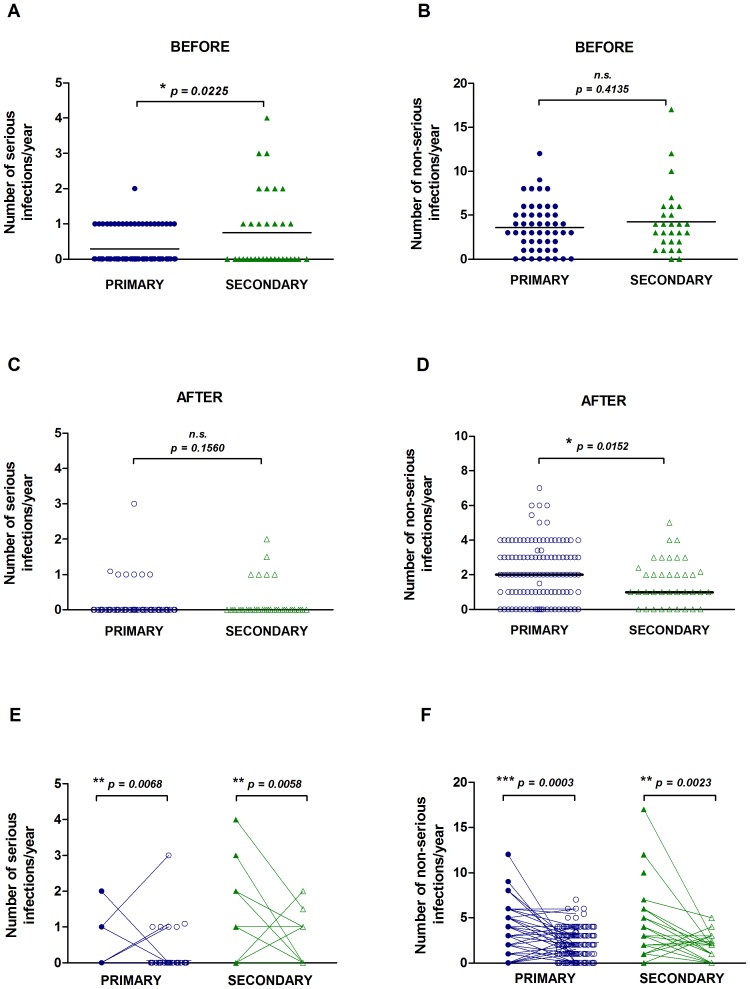
Secondary antibody deficiency can occur as a result of haematological malignancies or certain medications, but not much is known about the clinical and immunological features of this group of patients as a whole. Here we describe a cohort of 167 patients with primary or secondary antibody deficiencies on immunoglobulin (Ig)-replacement treatment. The demographics, causes of immunodeficiency, diagnostic delay, clinical and laboratory features, and infection frequency were analysed retrospectively. Chemotherapy for B cell lymphoma and the use of Rituximab, corticosteroids or immunosuppressive medications were the most common causes of secondary antibody deficiency in this cohort. There was no difference in diagnostic delay or bronchiectasis between primary and secondary antibody deficiency patients, and both groups experienced disorders associated with immune dysregulation. Secondary antibody deficiency patients had similar baseline levels of serum IgG, but higher IgM and IgA, and a higher frequency of switched memory B cells than primary antibody deficiency patients. Serious and non-serious infections before and after Ig-replacement were also compared in both groups. Although secondary antibody deficiency patients had more serious infections before initiation of Ig-replacement, treatment resulted in a significant reduction of serious and non-serious infections in both primary and secondary antibody deficiency patients. Patients with secondary antibody deficiency experience similar delays in diagnosis as primary antibody deficiency patients and can also benefit from immunoglobulin-replacement treatment.
Conflict of interest statement
Figures
References
-
- Castigli E, Geha RS (2006) Molecular basis of common variable immunodeficiency. J Allergy Clin Immunol 117: 740–746. - PubMed
-
- Duraisingham SS, Buckland MS, Grigoriadou S, Longhurst HJ (2014) Secondary antibody deficiency. Expert Rev Clin Immunol 10: 583–591. - PubMed
-
- Herriot R, Sewell WA (2008) Antibody deficiency. J Clin Pathol 61: 994–1000. - PubMed
-
- Rose ME, Lang DM (2006) Evaluating and managing hypogammaglobulinemia. Cleve Clin J Med 73: 133–137, 140, 143–134. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
