

The clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: a cohort of hospitalized patients
- PMID: 24971791
- PMCID: PMC4074190
- DOI: 10.1371/journal.pone.0101228
The clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: a cohort of hospitalized patients
Abstract
Background: Chronic Obstructive Pulmonary Disease (COPD) is a common disease with significant health and economic consequences. This study assesses the burden of COPD in the general population, and the influence of exacerbations (E-COPD) on disease progression and costs.
Methods: This is a secondary data analysis of healthcare administrative databases of the region of Lombardy, in northern Italy. The study included ≥ 40 year-old patients hospitalized for a severe E-COPD (index event) during 2006. Patients were classified in relation to the number and type of E-COPD experienced in a three-year pre-index period. Subjects were followed up until December 31st, 2009, collecting data on healthcare resource use and vital status.
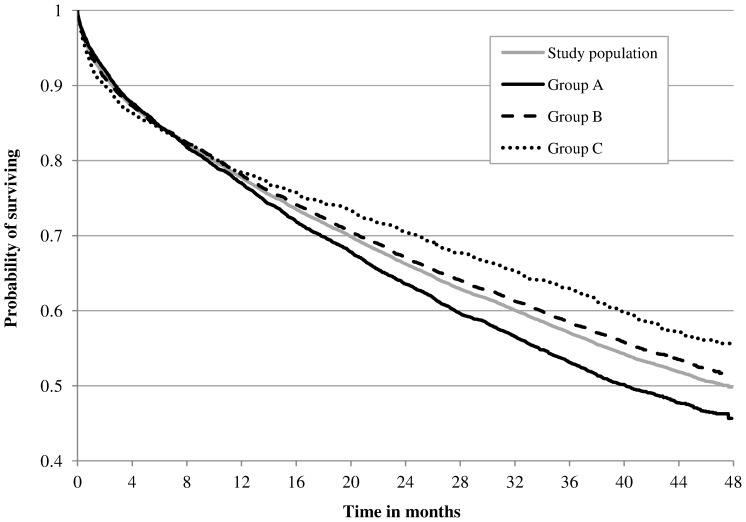
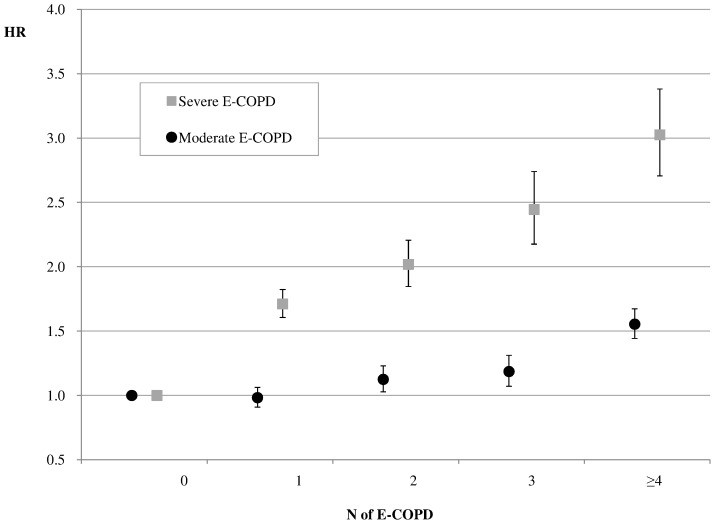
Results: 15857 patients were enrolled -9911 males, mean age: 76 years (SD 10). Over a mean follow-up time of 2.4 years (1.36), 81% of patients had at least one E-COPD with an annual rate of 3.2 exacerbations per person-year and an all-cause mortality of 47%. A history of exacerbation influenced the occurrence of new E-COPD and mortality after discharge for an E-COPD. On average, the healthcare system spent 6725€ per year per person (95%CI 6590-6863). Occurrence and type of exacerbations drove the direct healthcare cost. Less than one quarter of patients presented claims for pulmonary function tests.
Conclusions: COPD imposes a substantial burden on healthcare systems, mainly attributable to the type and occurrence of E-COPD, or in other words, to the exacerbator phenotypes. A more tailored approach to the management of COPD patients is required.
Conflict of interest statement
Figures

References
-
- (2007) Global surveillance, prevention and control of chronic respiratory disease. A comprehensive approach. In: Press W, editor. WHO Library Cataloguing. Switzerland: WHO.
-
- (2008) World Health Statistics 2008. WHO.
-
- Cazzola M, MacNee W, Martinez FJ, Rabe KF, Franciosi LG, et al. (2008) Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J 31: 416–469. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
