

An autopsy study of combined pulmonary fibrosis and emphysema: correlations among clinical, radiological, and pathological features
- PMID: 24972672
- PMCID: PMC4100038
- DOI: 10.1186/1471-2466-14-104
An autopsy study of combined pulmonary fibrosis and emphysema: correlations among clinical, radiological, and pathological features
Abstract
Background: Clinical evaluation to differentiate the characteristic features of pulmonary fibrosis and emphysema is often difficult in patients with combined pulmonary fibrosis and emphysema (CPFE), but diagnosis of pulmonary fibrosis is important for evaluating treatment options and the risk of acute exacerbation of interstitial pneumonia of such patients. As far as we know, it is the first report describing a correlation among clinical, radiological, and whole-lung pathological features in an autopsy cases of CPFE patients.
Methods: Experts retrospectively reviewed the clinical charts and examined chest computed tomography (CT) images and pathological findings of an autopsy series of 22 CPFE patients, and compared these with findings from 8 idiopathic pulmonary fibrosis (IPF) patients and 17 emphysema-alone patients.
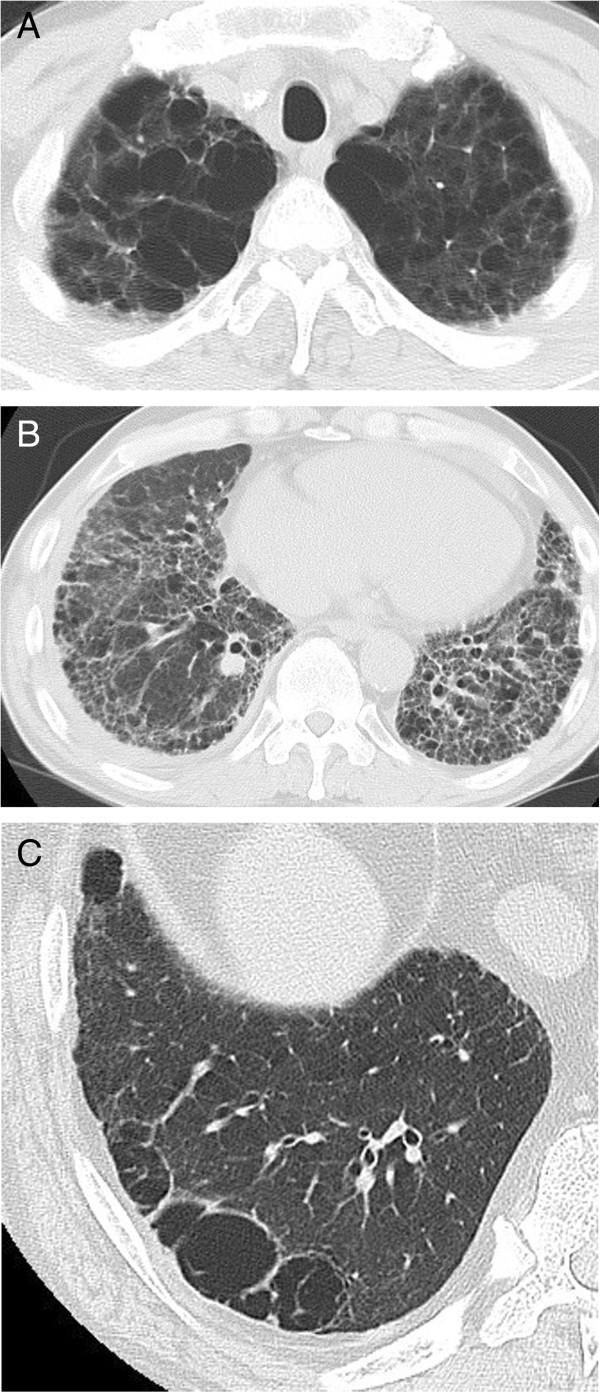
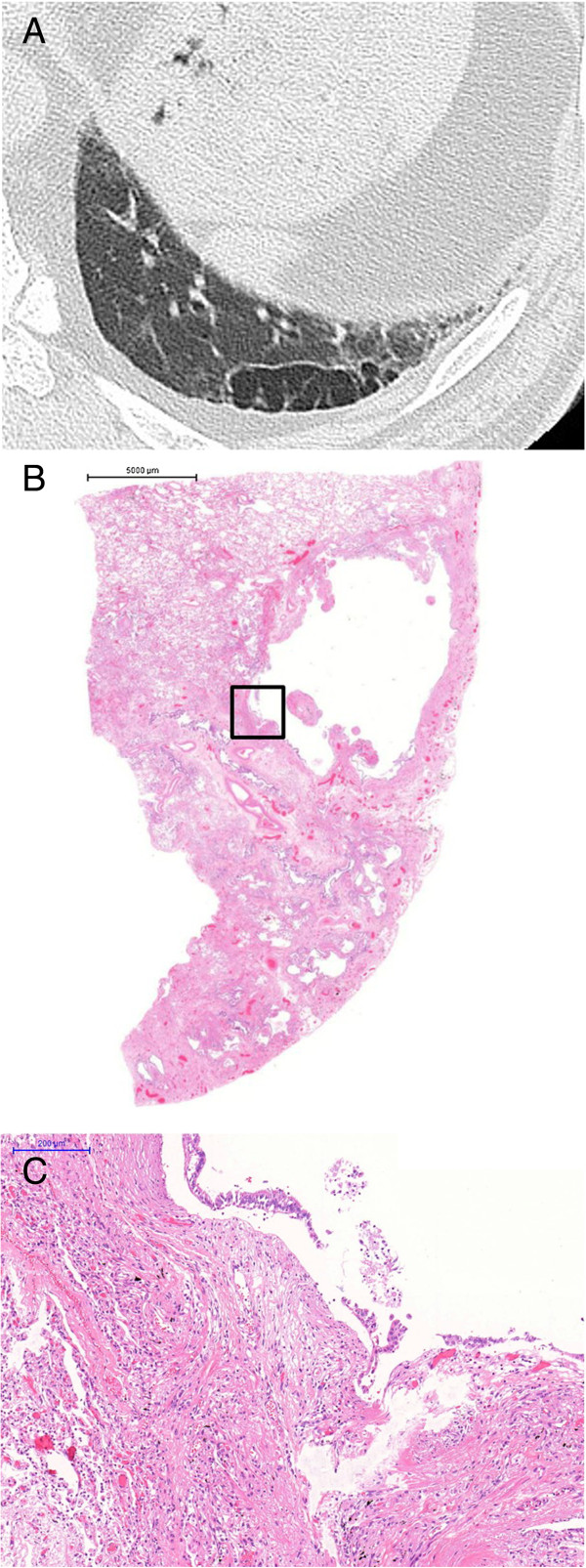
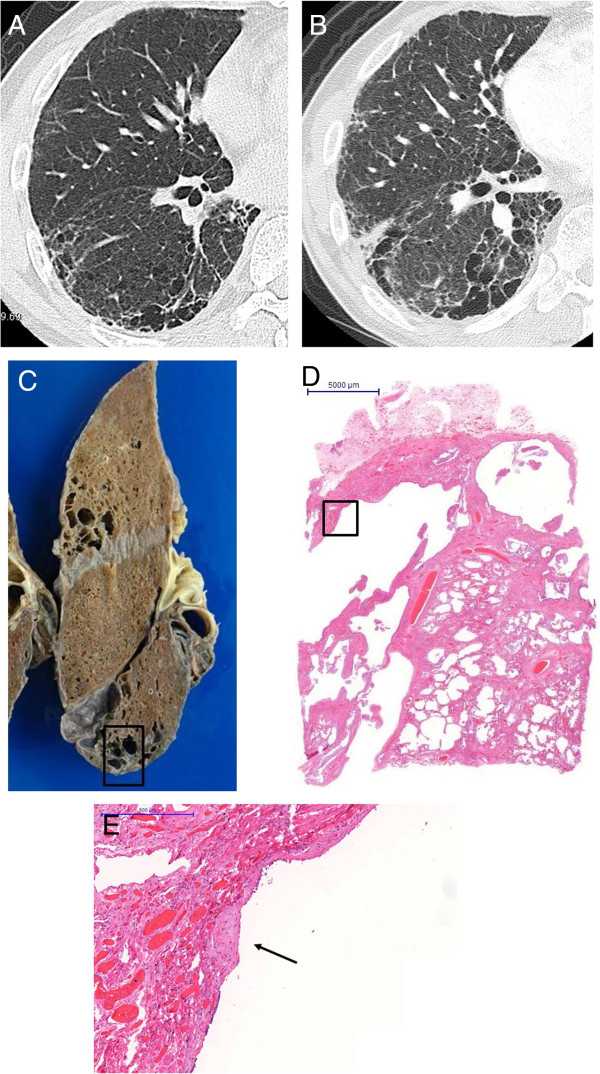
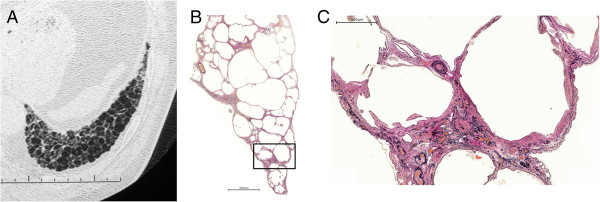
Results: All patients had a history of heavy smoking. Forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC%) was significantly lower in the emphysema-alone group than the CPFE and IPF-alone groups. The percent predicted diffusing capacity of the lung for carbon monoxide (DLCO%) was significantly lower in the CPFE group than the IPF- and emphysema-alone groups. Usual interstitial pneumonia (UIP) pattern was observed radiologically in 15 (68.2%) CPFE and 8 (100%) IPF-alone patients and was pathologically observed in all patients from both groups. Pathologically thick-cystic lesions involving one or more acini with dense wall fibrosis and occasional fibroblastic foci surrounded by honeycombing and normal alveoli were confirmed by post-mortem observation as thick-walled cystic lesions (TWCLs). Emphysematous destruction and enlargement of membranous and respiratory bronchioles with fibrosis were observed in the TWCLs. The cystic lesions were always larger than the cysts of honeycombing. The prevalence of both radiological and pathological TWCLs was 72.7% among CPFE patients, but no such lesions were observed in patients with IPF or emphysema alone (p=0.001). The extent of emphysema in CPFE patients with TWCLs was greater than that in patients without such lesions. Honeycombing with emphysema was also observed in 11 CPFE patients.
Conclusions: TWCLs were only observed in the CPFE patients. They were classified as lesions with coexistent fibrosing interstitial pneumonia and emphysema, and should be considered an important pathological and radiological feature of CPFE.
Figures

References
-
- Cottin V, Nunes H, Brillet PY, Delaval P, Devouassoux G, Tillie-Leblond I, Israel-Biet D, Court-Fortune I, Valeyre D, Cordier JF. Groupe d'Etude et de Recherche sur les Maladies Orphelines Pulmonaires (GERM O P) Combined pulmonary fibrosis and emphysema: a distinct underrecognised entity. Eur Respir J. 2005;26:586–593. doi: 10.1183/09031936.05.00021005. - DOI - PubMed
-
- Kawabata Y, Hoshi E, Murai K, Ikeya T, Takahashi N, Saitou Y, Kurashima K, Ubukata M, Takayanagi N, Sugita H, Kanauchi S, Colby TV. Smoking-related changes in the background lung of specimens resected for lung cancer: a semiquantitative study with correlation to postoperative course. Histopathology. 2008;53:707–714. doi: 10.1111/j.1365-2559.2008.03183.x. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
