

Role of cardiac evaluation before thoracic endovascular aortic repair
- PMID: 24973286
- PMCID: PMC4336174
- DOI: 10.1016/j.jvs.2014.05.029
Role of cardiac evaluation before thoracic endovascular aortic repair
Abstract
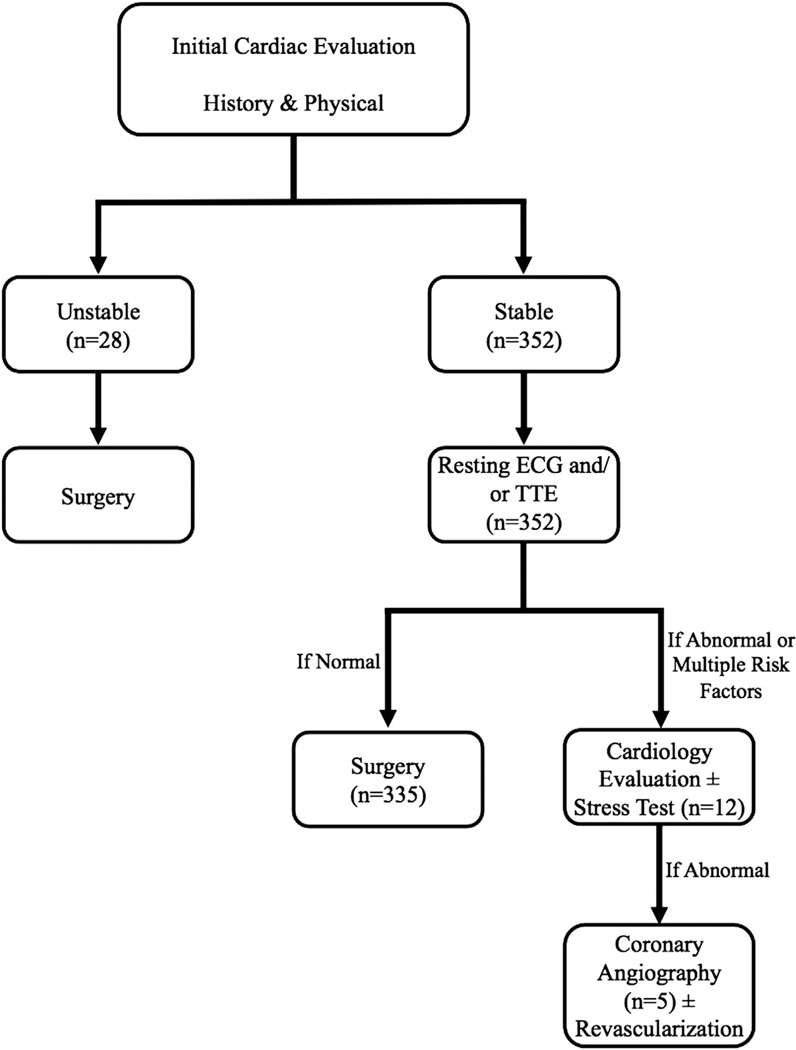
Background: Patients with thoracic aortic disease undergoing thoracic endovascular aortic repair (TEVAR) often have concomitant coronary artery disease and are at risk for perioperative adverse cardiac events. Despite this risk, the need for and extent of preoperative cardiac workup before TEVAR remain undefined. This study seeks to assess the adequacy of a limited cardiac evaluation before TEVAR, including assessment of cardiac symptoms, resting electrocardiography (ECG), and transthoracic echocardiography (TTE), as well as to estimate the incidence of perioperative cardiac events in patients undergoing TEVAR.
Methods: Retrospective analysis of a prospectively maintained Institutional Review Board-approved database was performed for all patients undergoing TEVAR at a single referral institution between May 2002 and June 2013. The analysis identified 463 TEVAR procedures. All procedures involving median sternotomy were excluded, and 380 procedures (343 patients) were included in the final analysis. Degree of cardiac workup was classified on the basis of the highest level of preoperative testing: no workup, resting ECG only, resting TTE, exercise/pharmacologic stress testing, or coronary angiography. Standard workup consisted of cardiac symptom assessment along with resting ECG or TTE, with further workup indicated for unstable symptoms, significantly abnormal findings on ECG or TTE, or multiple cardiac risk factors. Categorical and continuous variables were compared by Fisher's exact test and analysis of variance, respectively.
Results: No preoperative cardiac workup was performed for 28 patients (7.4%); 127 patients (33.4%) had resting ECG only, 208 patients (54.7%) had resting echocardiography, 12 patients (3.2%) underwent stress testing, and five patients (1.3%) had coronary angiography. Patients undergoing stress testing or coronary angiography were older and had a higher incidence of known coronary artery disease (P < .01) and prior myocardial infarction (P = .01). Complex hybrid aortic repairs and TEVAR for aneurysmal disease were more likely to have an extensive workup, whereas nonelective procedures more commonly had no workup. A total of nine patients (2.4%) experienced a perioperative cardiac event (myocardial infarction or cardiac arrest), with no significant difference noted among all groups (P = .45), suggesting that the extent of cardiac workup was appropriate. The incidence of 30-day/in-hospital mortality (5.5%) and cardiac-specific mortality (0.8%) was similar among all groups.
Conclusions: The risk of a postoperative cardiac event after TEVAR is low (2.4%), and initial screening with either resting TTE or ECG, in addition to assessment of cardiac symptom status, appears adequate for most TEVAR patients. As such, we recommend resting TTE or ECG as the initial cardiovascular screening mechanism in patients undergoing TEVAR, with subsequent more invasive studies if initial screening reveals cardiovascular abnormalities.
Copyright © 2014 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
Comment in
-
Discussion.J Vasc Surg. 2014 Nov;60(5):1203. doi: 10.1016/j.jvs.2014.05.030. Epub 2014 Jun 25. J Vasc Surg. 2014. PMID: 24973285 No abstract available.
References
-
- L’Italien GJ, Cambria RP, Cutler BS, Leppo JA, Paul SD, Brewster DC, et al. Comparative early and late cardiac morbidity among patients requiring different vascular surgery procedures. J Vasc Surg. 1995;21:935–944. - PubMed
-
- Omar HR, Mangar D, Camporesi EM. Preoperative cardiac evaluation of the vascular surgery patient—an anesthesia perspective. Vasc Endovascular Surg. 2012;46:201–211. - PubMed
-
- Troisi N, Dorigo W, Lo Sapio P, Pratesi G, Pulli R, Gensini GF, et al. Preoperative cardiac assessment in patients undergoing aortic surgery: analysis of factors affecting the cardiac outcomes. Ann Vasc Surg. 2010;24:733–740. - PubMed
-
- Back MR, Schmacht DC, Bowser AN, Stordahl N, Cuthbertson D, Johnson BL, et al. Critical appraisal of cardiac risk stratification before elective vascular surgery. Vasc Endovascular Surg. 2003;37:387–397. - PubMed
-
- Ferro CR, de Oliveira DC, Guerra Fde F, de Lucena AJ, Nunes FP, Ortiz ST, et al. Prevalence and risk factors for combined coronary artery disease and aortic aneurysm. Arq Bras Cardiol. 2007;88:40–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
