

Impact of catheter fragmentation followed by local intrapulmonary thrombolysis in acute high risk pulmonary embolism as primary therapy
- PMID: 24973834
- PMCID: PMC4121751
- DOI: 10.1016/j.ihj.2014.03.024
Impact of catheter fragmentation followed by local intrapulmonary thrombolysis in acute high risk pulmonary embolism as primary therapy
Abstract
Background: Pulmonary embolism (PE) with more than 50% compromise of pulmonary circulation results significant right ventricular (RV) afterload leading to progressive RV failure, systemic hypotension and shock. Prompt restoration of thrombolysis, surgical embolectomy, or percutaneous mechanical thrombectomy (PMT) prevents progressive hemodynamic decline. We report our single center experience in high risk PE patients treated with standard pigtail catheter mechanical fragmentation followed by intrapulmonary thrombolysis as a primary therapy.
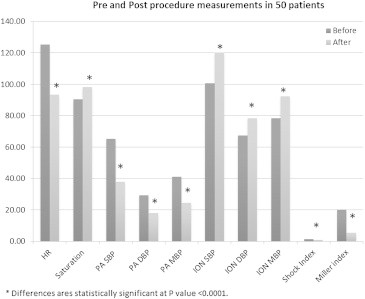
Methods: 50 consecutive patients with diagnosis of high risk PE defined as having shock index >1 with angiographic evidence of >50% pulmonary arterial occlusion are included in the present study. All patients underwent emergent cardiac catheterization. After ensuring flow across pulmonary artery with mechanical breakdown of embolus by rotating 5F pigtail catheter; bolus dose of urokinase (4400 IU/kg) followed by infusion for 24 h was given in the thrombus. Hemodynamic parameters were recorded and follow up pulmonary angiogram was done. Clinical and echo follow up was done for one year.
Results: Pigtail rotational mechanical thrombectomy restored antegrade flow in all patients. The mean pulmonary artery pressure, Miller score, Shock index decreased significantly from 41 ± 8 mmHg, 20 ± 5, 1.32 ± 0.3 to 24.52 ± 6.89, 5.35 ± 2.16, 0.79 ± 0.21 respectively (p < 0.0001). In-hospital major complications were seen in 4 patients. There was a statistically significant reduction of PA pressures from 62 ± 11 mmHg to 23±6 mmHg on follow up.
Conclusions: Rapid reperfusion of pulmonary arteries with mechanical fragmentation by pigtail catheter followed by intrapulmonary thrombolysis results in excellent immediate and intermediate term outcomes in patients presenting with high risk pulmonary embolism.
Keywords: Catheter fragmentation; Intrapulmonary; Pulmonary embolism; Thrombolysis.
Copyright © 2014. Published by Elsevier B.V.
Figures



Similar articles
-
Catheter-directed aspiration thrombectomy and low-dose thrombolysis for patients with acute unstable pulmonary embolism: Prospective outcomes from a PE registry.Int J Cardiol. 2019 Jul 15;287:106-110. doi: 10.1016/j.ijcard.2019.02.061. Epub 2019 Feb 28. Int J Cardiol. 2019. PMID: 30846255
-
Hybrid treatment of acute massive pulmonary thromboembolism: mechanical fragmentation with a modified rotating pigtail catheter, local fibrinolytic therapy, and clot aspiration followed by systemic fibrinolytic therapy.AJR Am J Roentgenol. 2004 Sep;183(3):589-95. doi: 10.2214/ajr.183.3.1830589. AJR Am J Roentgenol. 2004. PMID: 15333340
-
Percutaneous mechanical thrombectomy combined with catheter-directed thrombolysis in the treatment of acute pulmonary embolism and lower extremity deep venous thrombosis: A novel one-stop endovascular strategy.J Int Med Res. 2018 Feb;46(2):836-851. doi: 10.1177/0300060517729898. Epub 2017 Sep 20. J Int Med Res. 2018. PMID: 29239263 Free PMC article.
-
Interventional Treatment of Pulmonary Embolism.Circ Cardiovasc Interv. 2017 Feb;10(2):e004345. doi: 10.1161/CIRCINTERVENTIONS.116.004345. Circ Cardiovasc Interv. 2017. PMID: 28213377 Review.
-
Catheter-Directed Thrombolysis for Pulmonary Embolism: The State of Practice.Tech Vasc Interv Radiol. 2018 Jun;21(2):78-84. doi: 10.1053/j.tvir.2018.03.003. Epub 2018 Mar 8. Tech Vasc Interv Radiol. 2018. PMID: 29784125 Review.
Cited by
-
Treatment of the acute severe pulmonary embolism using endovascular methods.Pol J Radiol. 2018 Jun 1;83:e248-e252. doi: 10.5114/pjr.2018.76785. eCollection 2018. Pol J Radiol. 2018. PMID: 30627243 Free PMC article.
-
Efficacy and safety of hydro-mechanical defragmentation in intermediate- and high-risk pulmonary embolism.Egypt Heart J. 2021 Sep 25;73(1):84. doi: 10.1186/s43044-021-00204-2. Egypt Heart J. 2021. PMID: 34564780 Free PMC article.
-
Health risk stratification based on computed tomography pulmonary artery obstruction index for acute pulmonary embolism.Sci Rep. 2018 Dec 17;8(1):17897. doi: 10.1038/s41598-018-36115-7. Sci Rep. 2018. PMID: 30559454 Free PMC article.
-
Feasibility and safety of catheter-directed thrombolysis via superficial cubital vein for the treatment of acute massive and submassive pulmonary embolism.Postepy Kardiol Interwencyjnej. 2021 Dec;17(4):389-397. doi: 10.5114/aic.2021.112081. Epub 2021 Dec 29. Postepy Kardiol Interwencyjnej. 2021. PMID: 35126554 Free PMC article.
References
-
- Heit J.A., Silverstein M.D., Mohr D.N. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med. 1999;159:445–453. - PubMed
-
- Wood K.E. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002;121:877–905. - PubMed
-
- Goldhaber S.Z., Visani L., De Rosa M., for ICOPER Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Registry (ICOPER) Lancet. 1999;353:1386–1389. - PubMed
-
- Kucher N., Goldhaber S.Z. Management of massive pulmonary embolism. Circulation. 2005;112:e28–e32. - PubMed
-
- Uflacker R. Interventional therapy for pulmonary embolism. J Vasc Interv Radiol. 2001;12:147–164. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
