

Hirschsprung's disease in children: a five year experience at a university teaching hospital in northwestern Tanzania
- PMID: 24973940
- PMCID: PMC4083133
- DOI: 10.1186/1756-0500-7-410
Hirschsprung's disease in children: a five year experience at a university teaching hospital in northwestern Tanzania
Abstract
Background: Hirschsprung's disease (HD) is the commonest cause of functional intestinal obstruction in children and poses challenges to pediatricians and pediatric surgeons practicing in resource-limited countries. This study describes the clinical characteristics and outcome of management of this disease in our setting and highlights challenges associated with the care of these patients and proffer solutions for improved outcome.
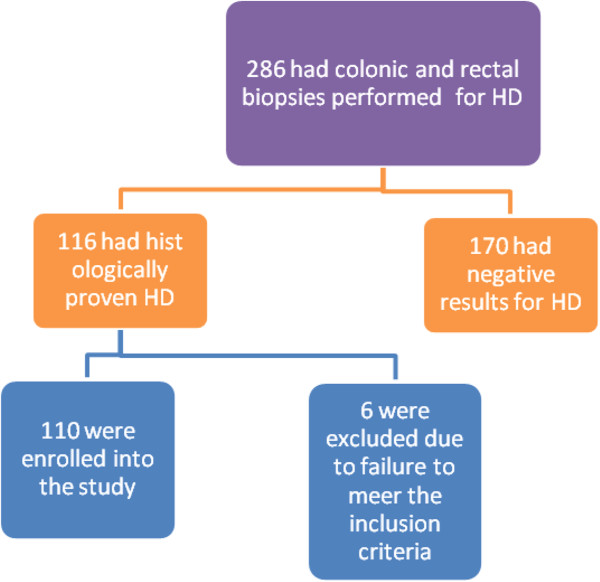
Methods: This was a descriptive prospective study of children aged ≤ 10 years who were histologically diagnosed and treated for HD at our centre between July 2008 and June 2013.
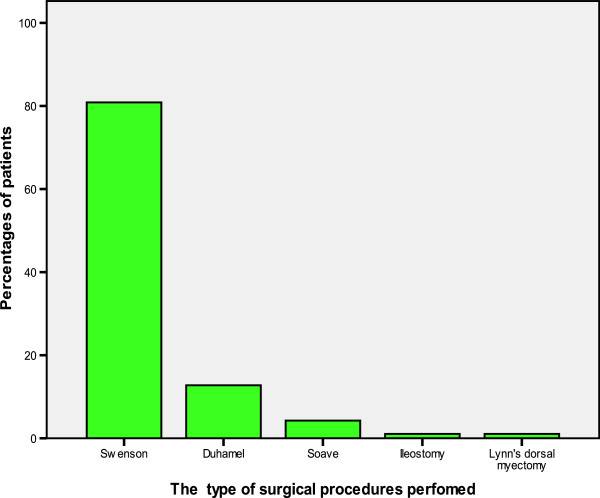
Results: A total of 110 patients (M: F ratio= 3.6:1) with a median age of 24 months were studied. Six (5.5%) patients were in the neonatal period. Sixty-four (58.2%) patients had complete intestinal obstruction whereas 42 (38.2%) and 4 (3.6%) patients had chronic intestinal obstruction and intestinal perforation respectively. No patient had enterocolitis. Constipation (94.5%) was the most common complaints. 109 (99.1%) patients had colostomy prior to the definitive pull-through. The median duration of colostomy before definitive pull-through was 4 months. The majority of patients (67.3%) had short segment of aganglionosis localized to the recto-sigmoid region. The definitive pull-through was performed in 94 (85.5%) patients (Swenson's pull-through 76 (80.9%), Duhamel's pull-through (12.8%) and Soave's pull-through 4 (4.3%) patients). Postoperative complication rate was 47.3%. The median length of hospital stay was 26 days. Patients who developed complications stayed longer in the hospital and this was statistically significant (p <0.001). Mortality rate was 21.8%. The age < 4 weeks, delayed presentation and surgical site infection were the main predictors of mortality (p < 0.001). During the follow-up period, the results of Swenson's and Duhamel's pull through procedures were generally good in 87.8% and 42.9% of patients respectively. The result of Soave's procedures was generally poor in this study.
Conclusion: HD remains the commonest cause of functional intestinal obstruction in children and contributes significantly to high morbidity and mortality in our setting. The majority of patients present late when the disease becomes complicated. Early diagnosis and timely definitive pull through procedure are essential in order to decrease the morbidity and mortality associated with this disease.
Figures
Similar articles
-
Management of Hirschsprung's disease: a comparison of Soave's and Duhamel's pull-through methods.Pediatr Surg Int. 2004 Aug;20(8):590-3. doi: 10.1007/s00383-004-1237-0. Epub 2004 Aug 11. Pediatr Surg Int. 2004. PMID: 15309470
-
Swenson's pull-through in older children and adults: peculiar peri-operative challenges of surgery.Int J Surg. 2011;9(8):652-4. doi: 10.1016/j.ijsu.2011.08.006. Epub 2011 Sep 16. Int J Surg. 2011. PMID: 21945674 Clinical Trial.
-
Swenson's operation for neonatal Hirschsprung's disease.Eur J Surg. 1993 Sep;159(9):487-9. Eur J Surg. 1993. PMID: 8274557
-
Management of Hirschsprung's disease: curative surgery before 3 months of age.J Pediatr Surg. 1989 Oct;24(10):1032-4. doi: 10.1016/s0022-3468(89)80209-x. J Pediatr Surg. 1989. PMID: 2681654 Review.
-
Primary laparoscopic endorectal pull-through for Hirschsprung's disease in infants and children.Semin Laparosc Surg. 1998 Mar;5(1):9-13. doi: 10.1177/155335069800500103. Semin Laparosc Surg. 1998. PMID: 9516554 Review.
Cited by
-
DIAGNOSTIC ACCURACY OF BARIUM ENEMA FINDINGS IN HIRSCHSPRUNG'S DISEASE.Arq Bras Cir Dig. 2016 Jul-Sep;29(3):155-158. doi: 10.1590/0102-6720201600030007. Arq Bras Cir Dig. 2016. PMID: 27759777 Free PMC article.
-
Diagnostic Role of Calretinin in Suspicious Cases of Hirschsprung's Disease.Cureus. 2021 Feb 16;13(2):e13373. doi: 10.7759/cureus.13373. Cureus. 2021. PMID: 33754098 Free PMC article.
-
Investigating colostomy-related morbidity in children following stoma formation and closure in a tertiary hospital, Abha, Saudi Arabia: a retrospective cohort study 2024.BMC Pediatr. 2024 Oct 3;24(1):630. doi: 10.1186/s12887-024-05089-z. BMC Pediatr. 2024. PMID: 39358702 Free PMC article.
-
Treatment and Patient Reported Outcome in Children with Hirschsprung Disease and Concomitant Congenital Heart Disease.Biomed Res Int. 2017;2017:1703483. doi: 10.1155/2017/1703483. Epub 2017 Mar 8. Biomed Res Int. 2017. PMID: 28373976 Free PMC article.
-
Fatal Toxic Megacolon in a Child of Hirschsprung Disease.J Clin Diagn Res. 2016 Dec;10(12):ED03-ED05. doi: 10.7860/JCDR/2016/21075.9083. Epub 2016 Dec 1. J Clin Diagn Res. 2016. PMID: 28208866 Free PMC article.
References
-
- Langer JC. In: Principle and Practice of Pediatric Surgery. 4. Colombani PM, Foglio RP, Skinner MA Oldham KT, editor. Philadelphia: Lippincott, Williams and Wilkins; 2005. p. 2. 1348-63.
-
- Teltelbaum DH, Coran AG. In: Hirschsprung’s Disease and Related Neuromuscular Disorders of the Intestine. 6. O’Neill JAJr, Fonkasrud EW, Coran AG Grosfeld JL, editor. Philadelphia: Mosby-Elservier; 2006. p. 2. 1514-59.
-
- Meza-Valencia BE, de Lorimier AJ, Person DA. Hirschsprung’s disease in the U.S. associated Pacific Islands: more common than expected. Hawaii Med J. 2005;64:96–98. - PubMed
-
- Feldmen M, Friedman LS, Sleisenger MH. Sleisenger & Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 7. Philadelphia, PA: Saunders; 2002. Hirschsprung’s disease: congenital megacolon; pp. 2131–2135.
-
- Stewart DR, von Allmen D. The genetics of Hirschsprung disease. Gastroenterol Clin North Am. 2003;32:819–837. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
