

Aggressive therapy for patients with non-small cell lung carcinoma and synchronous brain-only oligometastatic disease is associated with long-term survival
- PMID: 24974152
- PMCID: PMC4592138
- DOI: 10.1016/j.lungcan.2014.06.001
Aggressive therapy for patients with non-small cell lung carcinoma and synchronous brain-only oligometastatic disease is associated with long-term survival
Abstract
Objectives: Optimal therapy for patients with non-small cell lung carcinoma (NSCLC) presenting with synchronous brain-only oligometastases (SBO) is not well defined. We sought to analyze the effect of differing therapeutic paradigms in this subpopulation.
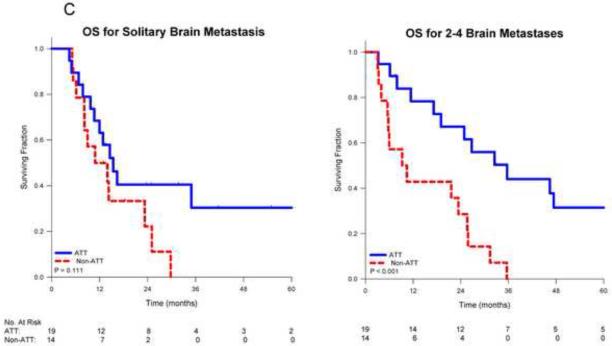
Materials and methods: We retrospectively analyzed NSCLC patients with 1-4 SBO diagnosed between 1/2000 and 1/2011 at our institution. Patients with T0 tumors or documented Karnofsky Performance Status <70 were excluded. Aggressive thoracic therapy (ATT) was defined as resection of the primary disease or chemoradiotherapy whose total radiation dose exceeded 45 Gy. Cox proportional hazards and competing risks models were used to analyze factors affecting survival and first recurrence in the brain.
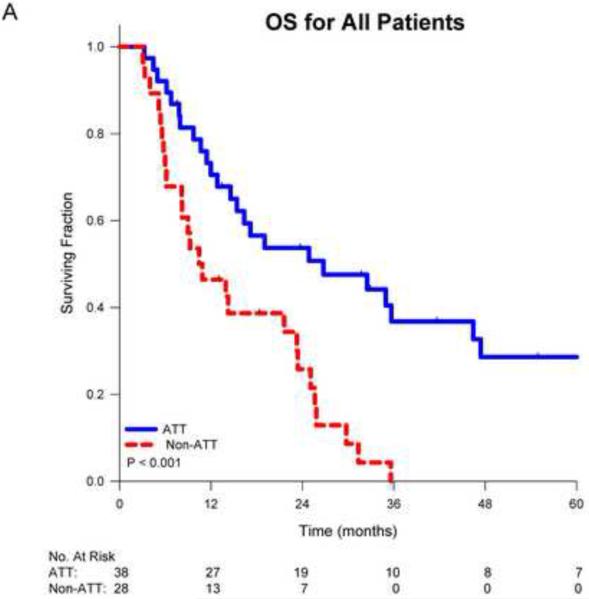
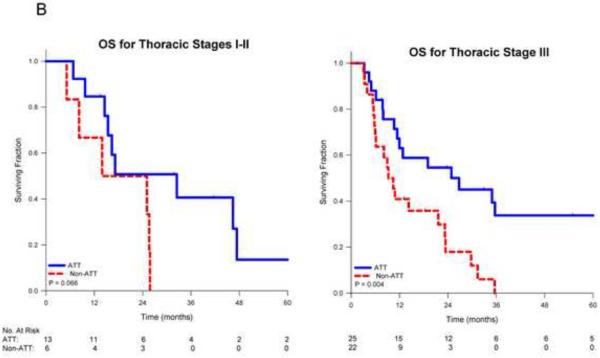
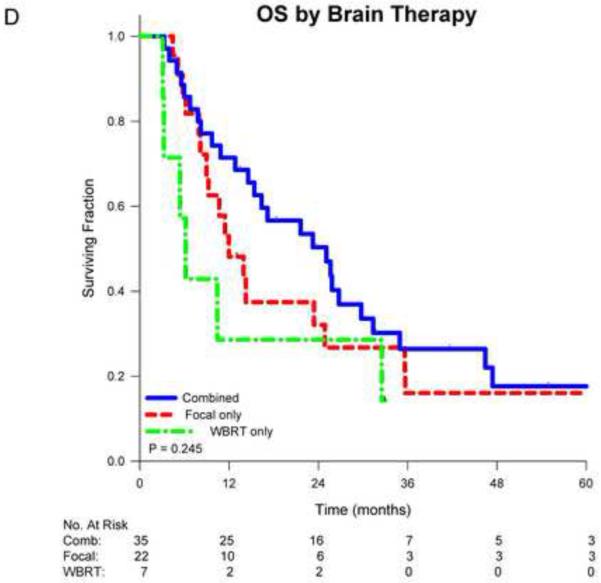
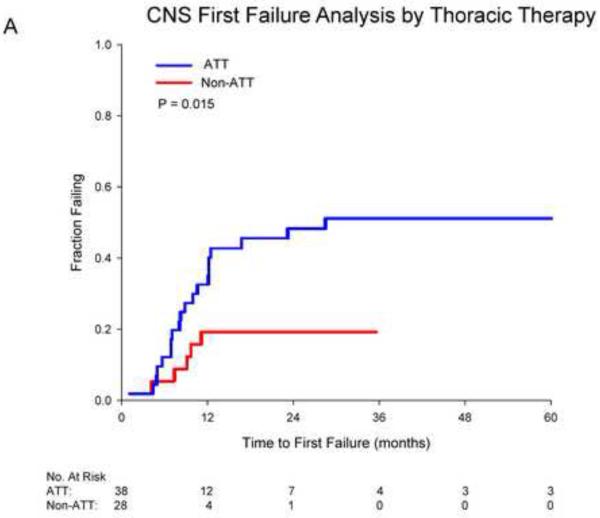
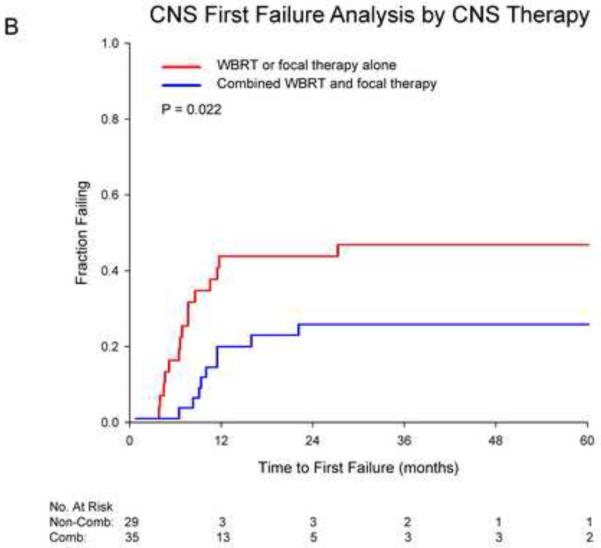
Results: Sixty-six patients were included. Median follow-up was 31.9 months. Intrathoracic disease extent included 9 stage I, 10 stage II and 47 stage III patients. Thirty-eight patients received ATT, 28 did not. Patients receiving ATT were younger (median age 55 vs. 60.5 years, p=0.027) but were otherwise similar to those who did not. Receipt of ATT was associated with prolonged median overall survival (OS) (26.4 vs. 10.5 months; p<0.001) with actuarial 2-year rates of 54% vs. 26%. ATT remained associated with OS after controlling for age, thoracic stage, performance status and initial brain therapy (HR 0.40, p=0.009). On multivariate analysis, the risk of first failure in the brain was associated with receipt of ATT (HR 3.62, p=0.032) and initial combined modality brain therapy (HR 0.34, p=0.046).
Conclusion: Aggressive management of thoracic disease in NSCLC patients with SBO is associated with improved survival. Careful management of brain disease remains important, especially for those treated aggressively.
Keywords: Aggressive therapy; Brain metastases; Non-small cell lung cancer; Oligometastases; Radiation therapy; Stereotactic radiosurgery; Whole brain radiotherapy.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol. 2004;22:2865–2872. - PubMed
-
- Billing PS, Miller DL, Allen MS, et al. Surgical treatment of primary lung cancer with synchronous brain metastases. J Thorac Cardiovasc Surg. 2001;122:548–553. - PubMed
-
- Bonnette P, Puyo P, Gabriel C, et al. Surgical management of non-small cell lung cancer with synchronous brain metastases. Chest. 2001;119:1469–1475. - PubMed
-
- Chidel MA, Suh JH, Greskovich JF, et al. Treatment outcome for patients with primary nonsmall-cell lung cancer and synchronous brain metastasis. Radiat Oncol Investig. 1999;7:313–319. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
