

Continuous versus bolus intermittent loop diuretic infusion in acutely decompensated heart failure: a prospective randomized trial
- PMID: 24974232
- PMCID: PMC4227080
- DOI: 10.1186/cc13952
Continuous versus bolus intermittent loop diuretic infusion in acutely decompensated heart failure: a prospective randomized trial
Abstract
Introduction: Intravenous loop diuretics are a cornerstone of therapy in acutely decompensated heart failure (ADHF). We sought to determine if there are any differences in clinical outcomes between intravenous bolus and continuous infusion of loop diuretics.
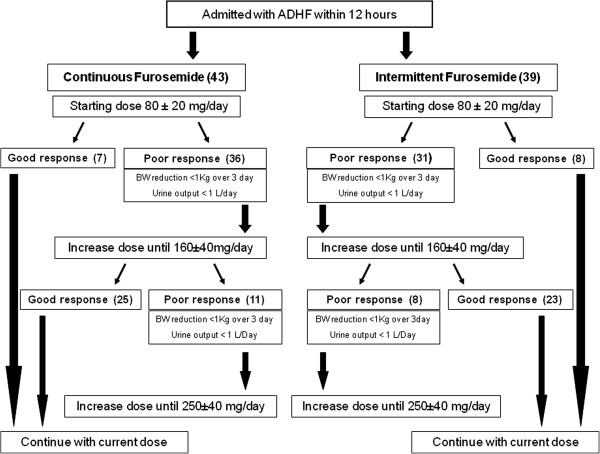
Methods: Subjects with ADHF within 12 hours of hospital admission were randomly assigned to continuous infusion or twice daily bolus therapy with furosemide. There were three co-primary endpoints assessed from admission to discharge: the mean paired changes in serum creatinine, estimated glomerular filtration rate (eGFR), and reduction in B-type natriuretic peptide (BNP). Secondary endpoints included the rate of acute kidney injury (AKI), change in body weight and six months follow-up evaluation after discharge.
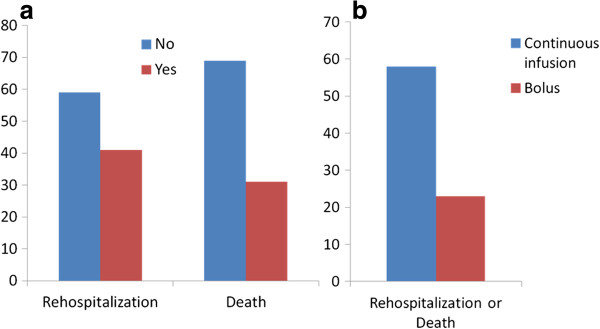
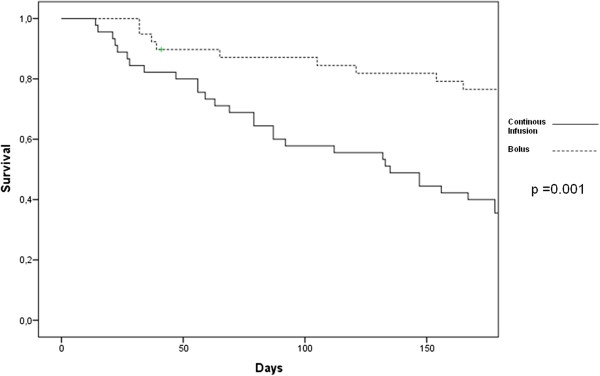
Results: A total of 43 received a continuous infusion and 39 were assigned to bolus treatment. At discharge, the mean change in serum creatinine was higher (+0.8 ± 0.4 versus -0.8 ± 0.3 mg/dl P <0.01), and eGFR was lower (-9 ± 7 versus +5 ± 6 ml/min/1.73 m(2) P <0.05) in the continuous arm. There was no significant difference in the degree of weight loss (-4.1 ± 1.9 versus -3.5 ± 2.4 kg P = 0.23). The continuous infusion arm had a greater reduction in BNP over the hospital course, (-576 ± 655 versus -181 ± 527 pg/ml P = 0.02). The rates of AKI were comparable (22% and 15% P = 0.3) between the two groups. There was more frequent use of hypertonic saline solutions for hyponatremia (33% versus 18% P <0.01), intravenous dopamine infusions (35% versus 23% P = 0.02), and the hospital length of stay was longer in the continuous infusion group (14. 3 ± 5 versus 11.5 ± 4 days, P <0.03). At 6 months there were higher rates of re-admission or death in the continuous infusion group, 58% versus 23%, (P = 0.001) and this mode of treatment independently associated with this outcome after adjusting for baseline and intermediate variables (adjusted hazard ratio = 2.57, 95% confidence interval, 1.01 to 6.58 P = 0.04).
Conclusions: In the setting of ADHF, continuous infusion of loop diuretics resulted in greater reductions in BNP from admission to discharge. However, this appeared to occur at the consequence of worsened renal filtration function, use of additional treatment, and higher rates of rehospitalization or death at six months.
Trial registration: ClinicalTrials.gov NCT01441245. Registered 23 September 2011.
Figures
Comment in
-
Intravenous furosemide in decompensated heart failure: do not protocolize dosing but the desired effect!Crit Care. 2014 Dec 22;18(6):709. doi: 10.1186/s13054-014-0709-4. Crit Care. 2014. PMID: 25672666 Free PMC article. No abstract available.
References
-
- Gupta S, Neyses L. Diuretic usage in heart failure: a continuing conundrum in 2005. Eur Heart J. 2005;26:644–649. - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Køber L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rønnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A, Bax JJ, Baumgartner H, Ceconi C. ESC Committee for Practice Guidelines (CPG) et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–1847. - PubMed
-
- Chuen MJ, MacFadyen RJ. Dose-dependent association between use of loop diuretics and mortality in advanced systolic heart failure. Am J Cardiol. 2006;98:1416–1417. - PubMed
-
- Abdel-Qadir HM, Tu JW, Yun L, Austin PC, Newton GE, Lee DS. Diuretic dose and long-term outcome in elderly patients with heart failure after hospitalization. Am Heart J. 2010;160:264–271. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
