

Presence of Candida cell wall derived polysaccharides in the sera of intensive care unit patients: relation with candidaemia and Candida colonisation
- PMID: 24975380
- PMCID: PMC4227034
- DOI: 10.1186/cc13953
Presence of Candida cell wall derived polysaccharides in the sera of intensive care unit patients: relation with candidaemia and Candida colonisation
Abstract
Introduction: Prompt diagnosis of candidaemia and invasive candidosis is crucial to the early initiation of antifungal therapy. The poor sensitivity of blood cultures (BCs) has led to the development of fungal glycan tests as a diagnostic adjunct. We analysed the performance of tests for the detection of circulating β-D-1,3-glucan (BDG) and mannan in the intensive care unit (ICU) setting.
Methods: This retrospective, case-control study included 43 ICU patients with candidaemia and 67 controls, hospitalised on the same ward and assessed weekly for yeast colonisation with simultaneous serum sampling; 340 sera taken before and after positive BCs were available for the cases group and 203 for the controls. BDG and mannan levels were determined using the Fungitell® and Platelia™ Candida Ag tests, respectively.
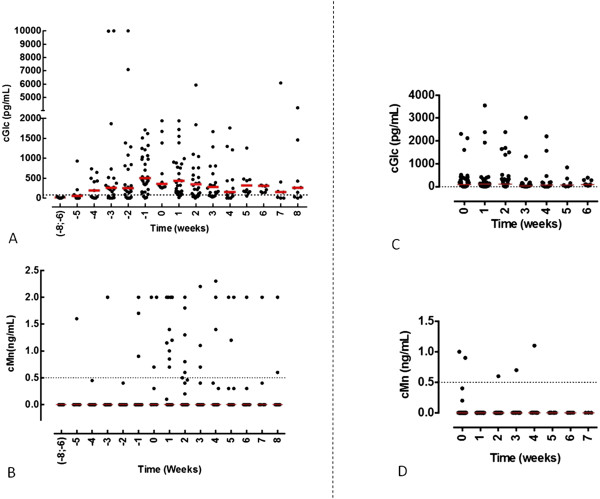
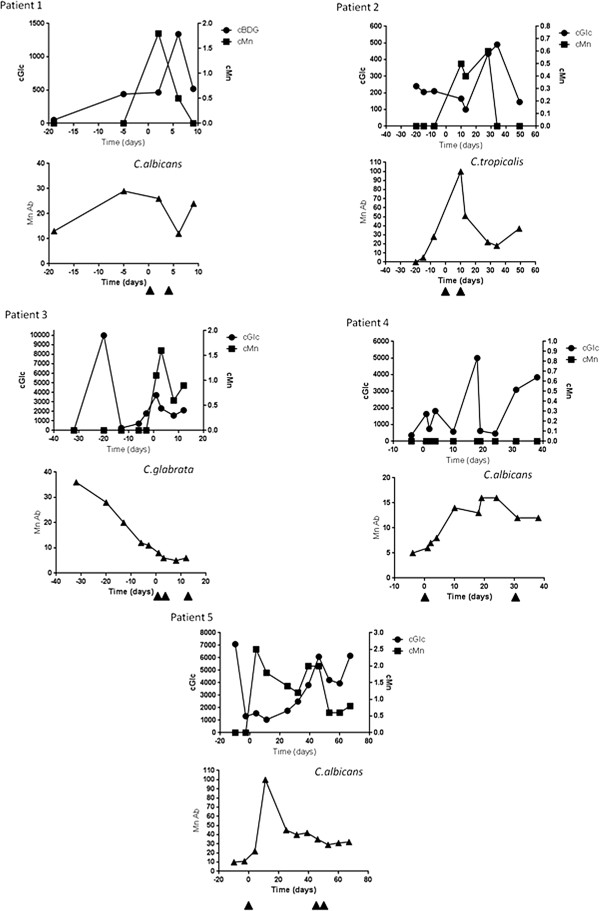
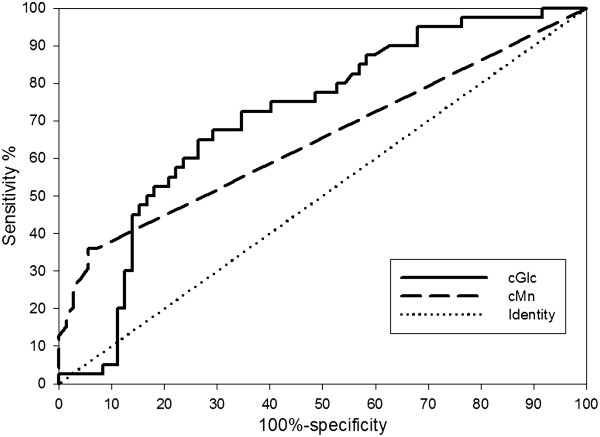
Results: BDG was detected early in sera from cases patients but was also present in several sera from controls. Increasing the cut-off from 80 pg/mL to 350 pg/mL and 800 pg/mL resulted in sensitivity/specificity ratios of 0.97/0.31, 0.65/0.74, 0.30/0.86, respectively. Detection of mannan was more specific but lacked sensitivity. No obvious correlation was found between BDG and colonisation, but a trend existed between high colonisation and high BDG. Candidaemia relapses were associated with a rise in BDG and mannan but, in contrast to the transient nature of mannan, BDG persisted up to 7 weeks after positive BCs.
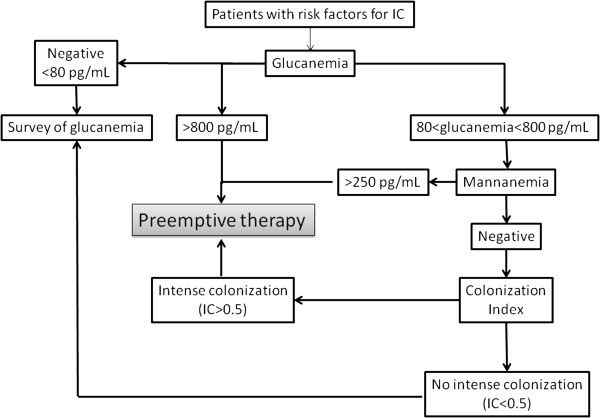
Conclusion: A combination of mannan and BDG tests could be used to guide pre-emptive therapeutic decisions in ICU patients.
Figures
References
-
- Morrell M, Fraser VJ, Kollef MH. Delaying the empiric treatment of candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother. 2005;49:3640–3645. doi: 10.1128/AAC.49.9.3640-3645.2005. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
