

Prospective randomized trial of venous angioplasty in MS (PREMiSe)
- PMID: 24975855
- PMCID: PMC4132574
- DOI: 10.1212/WNL.0000000000000638
Prospective randomized trial of venous angioplasty in MS (PREMiSe)
Erratum in
- Neurology. 2014 Aug 19;83(8):773
Abstract
Objective: We report the results of the investigation of safety and efficacy of venous angioplasty in patients with multiple sclerosis (MS) with findings of extracranial venous anomalies, considered hallmarks of chronic cerebrospinal venous insufficiency (CCSVI), in a 2-phase study (ClinicalTrials.gov NCT01450072).
Methods: Phase 1 was an open-label safety study (10 patients); phase 2 was sham-controlled, randomized, and double-blind (10 sham procedure, 9 treated). All study patients fulfilled venous hemodynamic screening criteria indicative of CCSVI. Assessment was at 1, 3, and 6 months postprocedure with MRI, clinical, and hemodynamic outcomes. Primary endpoints were safety at 24 hours and 1 month, venous outflow restoration >75% at 1 month, and effect of angioplasty on new lesion activity and relapse rate over 6 months. Secondary endpoints included changes in disability, brain volume, cognitive tests, and quality of life.
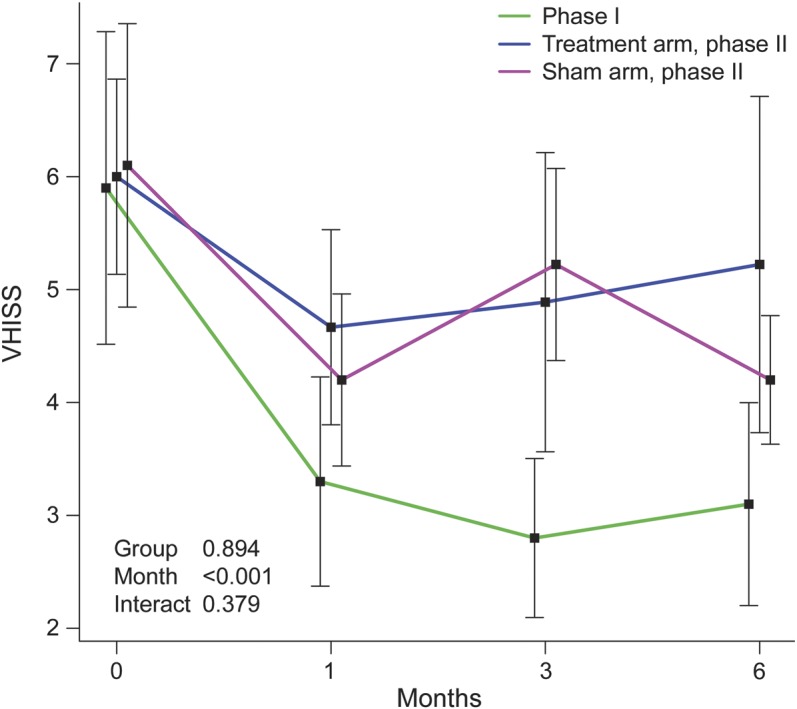
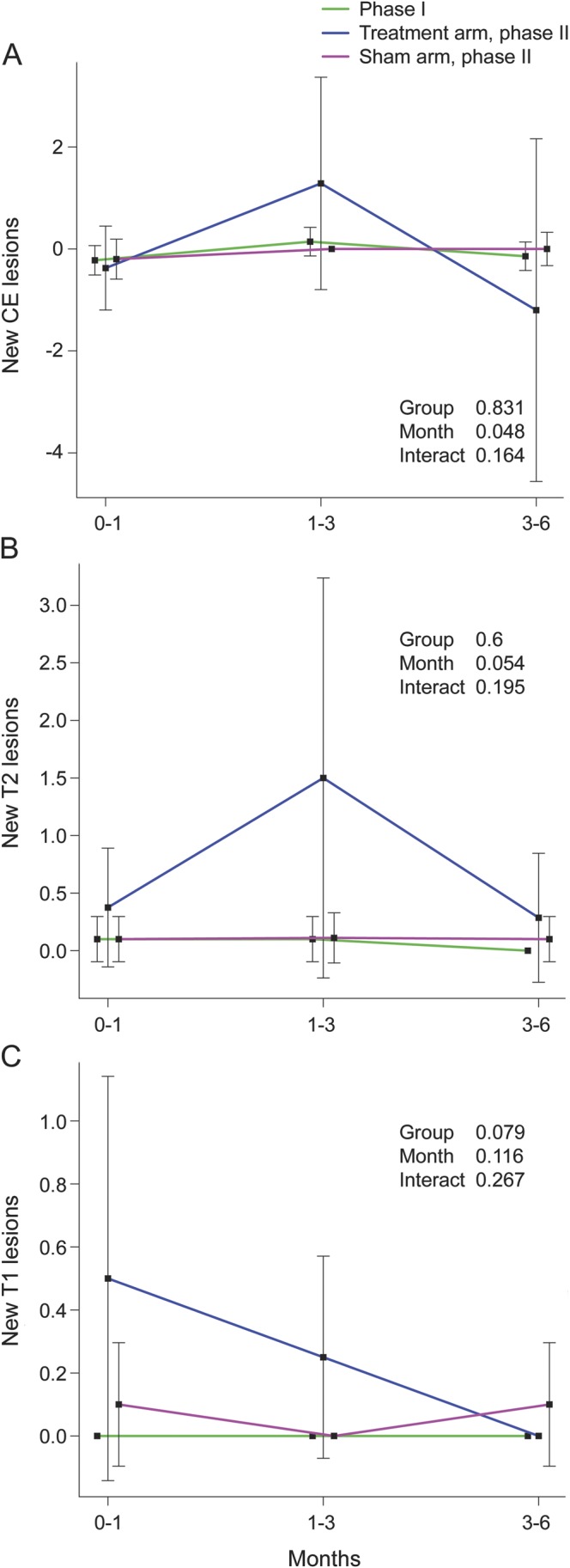
Results: No perioperative complications were noted; however, one patient with history of syncope was diagnosed with episodic bradycardia requiring placement of a pacemaker before discharge. Doppler evidence-based venous hemodynamic insufficiency severity score (VHISS) was reduced >75% compared to baseline in phase 1 (at 1 month) but not phase 2. In phase 2, higher MRI activity (cumulative number of new contrast-enhancing lesions [19 vs 3, p = 0.062] and new T2 lesions [17 vs 3, p = 0.066]) and relapse activity (4 vs 1, p = 0.389) were identified as nonsignificant trends in the treated vs sham arm over 6 months. Using analysis of covariance, significant cumulative new T2 lesions were related to larger VHISS decrease (p = 0.028) and angioplasty (p = 0.01) over the follow-up. No differences in other endpoints were detected.
Conclusion: Venous angioplasty is not an effective treatment for MS over the short term and may exacerbate underlying disease activity.
Classification of evidence: This is a Class I study demonstrating that clinical and imaging outcomes are no better or worse in patients with MS identified with venous outflow restriction who receive venous angioplasty compared to sham controls who do not receive angioplasty. This study also includes a Class IV phase 1 study of safety in 10 patients receiving the angioplasty procedure.
© 2014 American Academy of Neurology.
Figures
Comment in
-
Venous angioplasty for "CCSVI" in multiple sclerosis: ending a therapeutic misadventure.Neurology. 2014 Jul 29;83(5):388-9. doi: 10.1212/WNL.0000000000000651. Epub 2014 Jun 27. Neurology. 2014. PMID: 24975856 No abstract available.
References
-
- Baracchini C, Perini P, Calabrese M, Causin F, Rinaldi F, Gallo P. No evidence of chronic cerebrospinal venous insufficiency at multiple sclerosis onset. Ann Neurol 2011;69:90–99 - PubMed
-
- Baracchini C, Perini P, Causin F, Calabrese M, Rinaldi F, Gallo P. Progressive multiple sclerosis is not associated with chronic cerebrospinal venous insufficiency. Neurology 2011;77:844–850 - PubMed
-
- Doepp F, Paul F, Valdueza JM, Schmierer K, Schreiber SJ. No cerebrocervical venous congestion in patients with multiple sclerosis. Ann Neurol 2010;68:173–183 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials