

Endovascular treatment in spinal perimedullary arteriovenous fistula
- PMID: 24976100
- PMCID: PMC4178764
- DOI: 10.15274/INR-2014-10056
Endovascular treatment in spinal perimedullary arteriovenous fistula
Abstract
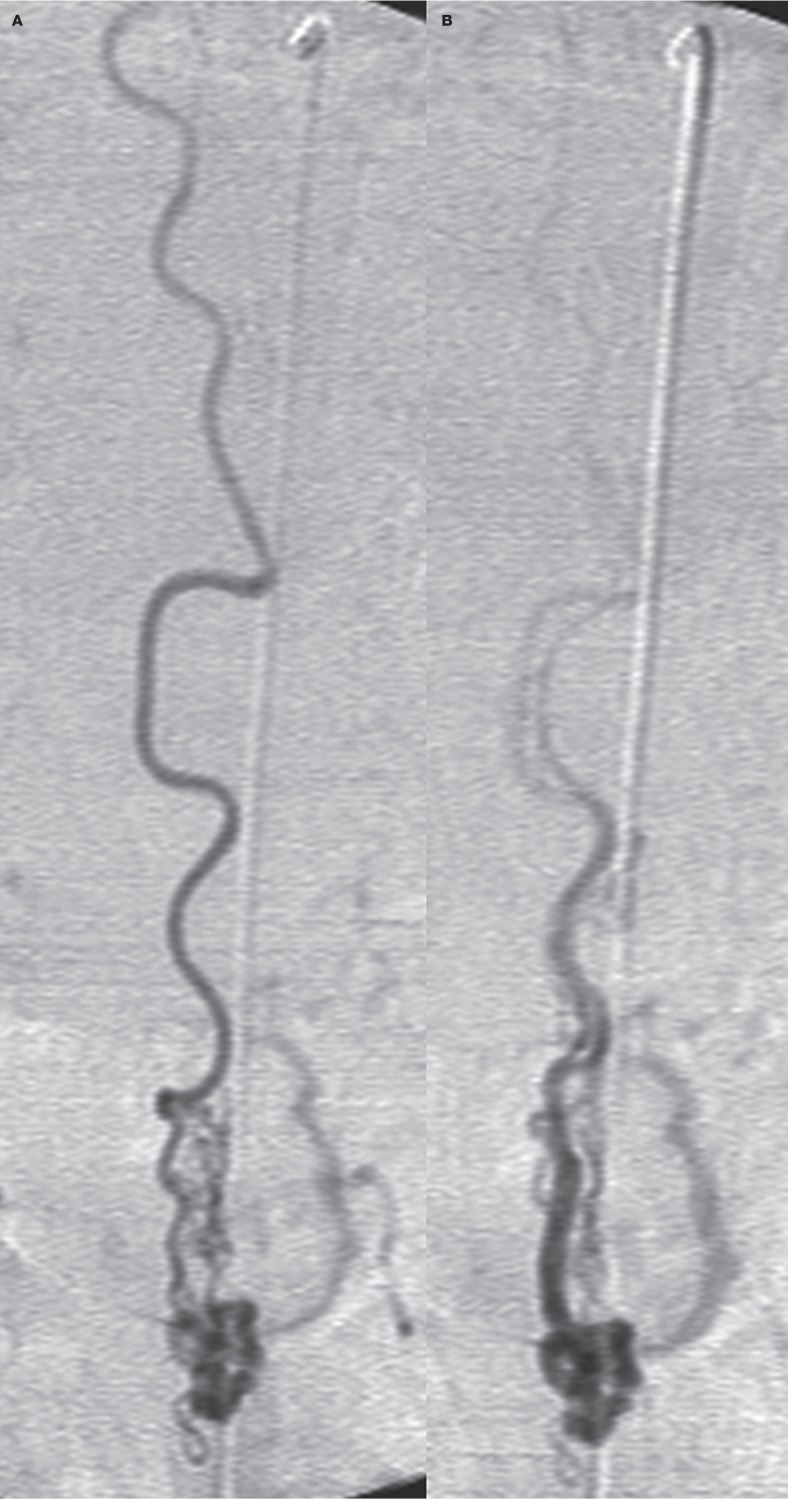
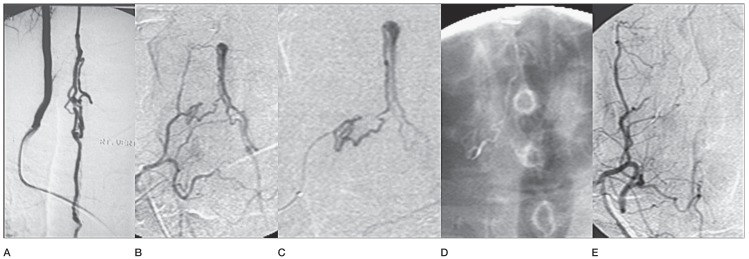
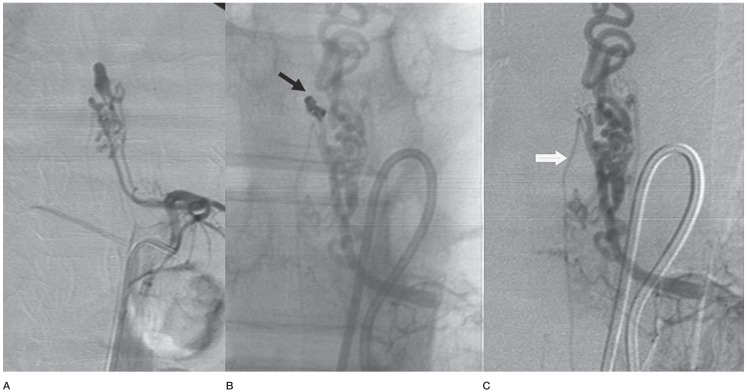
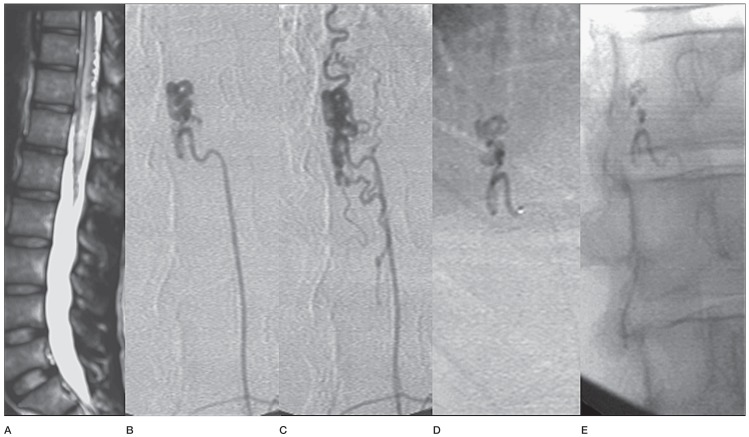
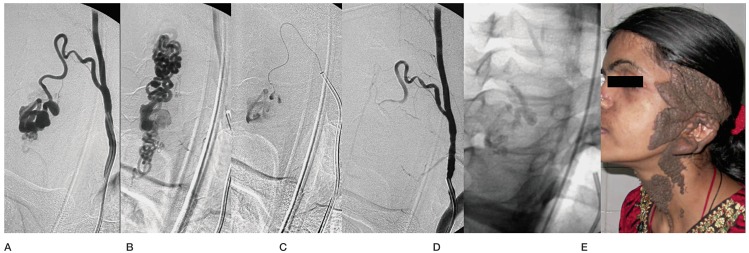
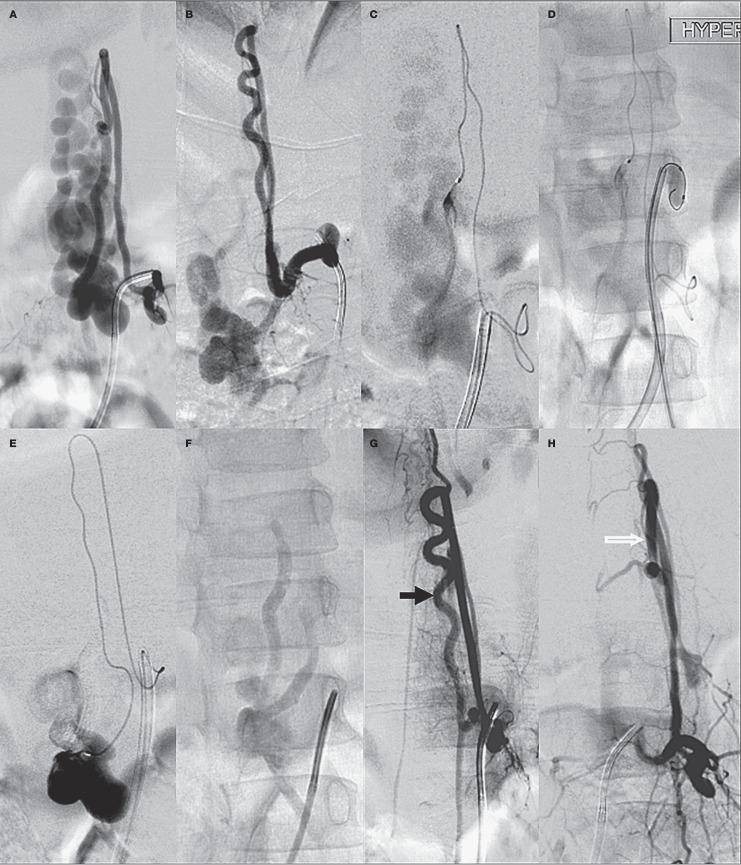
This study includes 20 patients with 21 spinal perimedullary fistulae. There were nine Type IVa (42.8%) lesions, ten Type IVb (47.6%) and two Type IVc (9.5%) lesions. The dominant arterial supply was from the anterior spinal artery (47.6%), posterior spinal artery (19%) and directly from the radiculomedullary artery (28.5%). Sixteen lesions in 15 patients were treated by endovascular route using n-butyl-2-cyanoacrylate. Endovascular treatment was not feasible in five patients. Of the ten patients with microfistulae, catheterization failed/was not attempted in 40%, complete obliteration of the lesion was seen in 60% but clinical improvement was seen in 40% of patients. Catheterization was feasible in all ten patients with macrofistulae (nine type IVb and two type IVc lesions). Complete obliteration of the lesions was seen in 60% and residue in 30%. Clinical improvement was seen in 80% and clinical deterioration in 10%. In conclusion, endovascular glue embolization is safe and efficacious in type IVb and IVc spinal perimedullary fistulae and should be considered the first option of treatment. It is also feasible in many of the type IVa lesions.
Keywords: embolization; perimedullary arteriovenous fistula; spinal cord.
Figures

Similar articles
-
Treatment of spinal cord perimedullary arteriovenous fistula: embolization versus surgery.Neurosurgery. 2005 Feb;56(2):232-41; discussion 232-41. doi: 10.1227/01.neu.0000147974.79671.83. Neurosurgery. 2005. PMID: 15670371 Review.
-
Pediatric perimedullary arteriovenous fistula: clinical features and endovascular treatments.J Neurointerv Surg. 2019 Apr;11(4):411-415. doi: 10.1136/neurintsurg-2018-014184. Epub 2018 Sep 27. J Neurointerv Surg. 2019. PMID: 30262658
-
Endovascular embolization for symptomatic perimedullary AVF and intramedullary AVM: a series and a literature review.Neuroradiology. 2012 Apr;54(4):349-59. doi: 10.1007/s00234-011-0880-0. Epub 2011 May 10. Neuroradiology. 2012. PMID: 21556862
-
Clinical features and treatment outcomes of the spinal arteriovenous fistulas and malformation: clinical article.J Neurosurg Spine. 2013 Aug;19(2):207-16. doi: 10.3171/2013.4.SPINE12732. Epub 2013 May 24. J Neurosurg Spine. 2013. PMID: 23705629
-
Endovascular treatment of spinal arteriovenous lesions: beyond the dural fistula.AJNR Am J Neuroradiol. 2011 May;32(5):798-808. doi: 10.3174/ajnr.A2190. Epub 2010 Jul 22. AJNR Am J Neuroradiol. 2011. PMID: 20651018 Free PMC article. Review.
Cited by
-
An unusual cause of vertigo and headache in childhood.Wien Med Wochenschr. 2017 Sep;167(11-12):282-284. doi: 10.1007/s10354-017-0581-3. Epub 2017 Jul 28. Wien Med Wochenschr. 2017. PMID: 28755020 English.
-
Single hole, high-flow, spinal cord peri-medullary arteriovenous fistula (PMAVF) in a child, treated with transarterial embolization: A case report.Radiol Case Rep. 2024 Jun 15;19(9):3661-3666. doi: 10.1016/j.radcr.2024.05.060. eCollection 2024 Sep. Radiol Case Rep. 2024. PMID: 38983308 Free PMC article.
-
Dorsal intradural spinal arteriovenous fistula associated with giant intradural spinal aneurysm, a case report.Clin Case Rep. 2023 Apr 13;11(4):e7202. doi: 10.1002/ccr3.7202. eCollection 2023 Apr. Clin Case Rep. 2023. PMID: 37064730 Free PMC article.
-
Study and therapeutic progress on spinal cord perimedullary arteriovenous fistulas.Biomed Rep. 2017 Sep;7(3):214-220. doi: 10.3892/br.2017.951. Epub 2017 Jul 25. Biomed Rep. 2017. PMID: 28808569 Free PMC article.
-
Microsurgical resection of a perimedullary conus medullaris arteriovenous fistula type IVa: a case report.Ann Med Surg (Lond). 2025 Jan 9;87(1):351-354. doi: 10.1097/MS9.0000000000002786. eCollection 2025 Jan. Ann Med Surg (Lond). 2025. PMID: 40109586 Free PMC article.
References
-
- Rodesch G, Hurth M, Alvarez H, et al. Spinal cord intradural arteriovenous fistulae: anatomic, clinical, and therapeutic considerations in a series of 32 consecutive patients seen between 1981 and 2000 with emphasis on endovascular therapy. Neurosurgery. 2005;57:973–981. doi: 10.1227/01.NEU.0000181314.94000.CD. - DOI - PubMed
-
- Hurst RW. Vascular disorders of the spine and spinal cord. In: Atlas SW, editor. Magnetic resonance imaging of the brain and spine. 3rd edn. Philadelphia: Lippincott Williams and Wilkins; 2002. pp. 1825–1854.
-
- Aydin K, Sencer S, Sencer A, et al. Angiography-induced closure of perimedullary spinal arteriovenous ?stula. Br J Radiol. 2004;77:969–973. doi: 10.1259/bjr/30760081. - DOI - PubMed
-
- Djindjian M, Djindjian R, Rey A, et al. Intradural extramedullay spinal arteriovenous malformations fed by the anterior spinal artery. Surg Neurol. 1977;2(2):85–93. - PubMed
-
- Heros RC, Debrun GM, Ojemann RG, et al. Direct spinal ateriovenous fistula: a new type of spinal AVM. J Neurosurg. 1986;64(1):134–139. doi: 10.3171/jns.1986.64.1.0134. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
