

Temporomandibular disorders. Part 1: anatomy and examination/diagnosis
- PMID: 24976743
- PMCID: PMC4062347
- DOI: 10.1179/2042618613Y.0000000060
Temporomandibular disorders. Part 1: anatomy and examination/diagnosis
Abstract
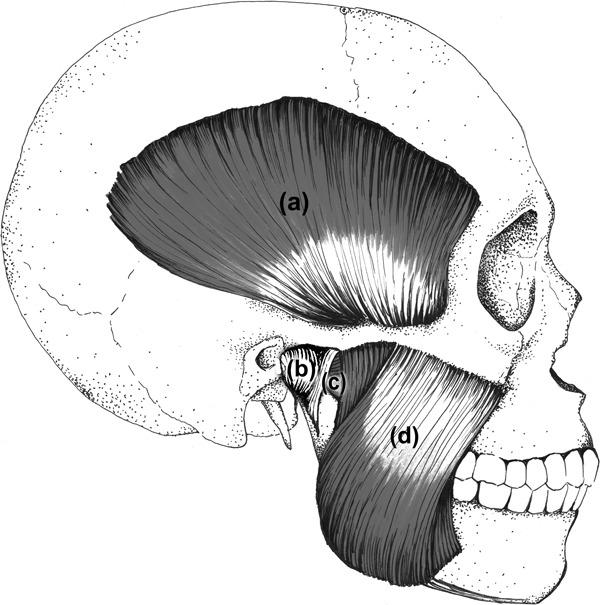
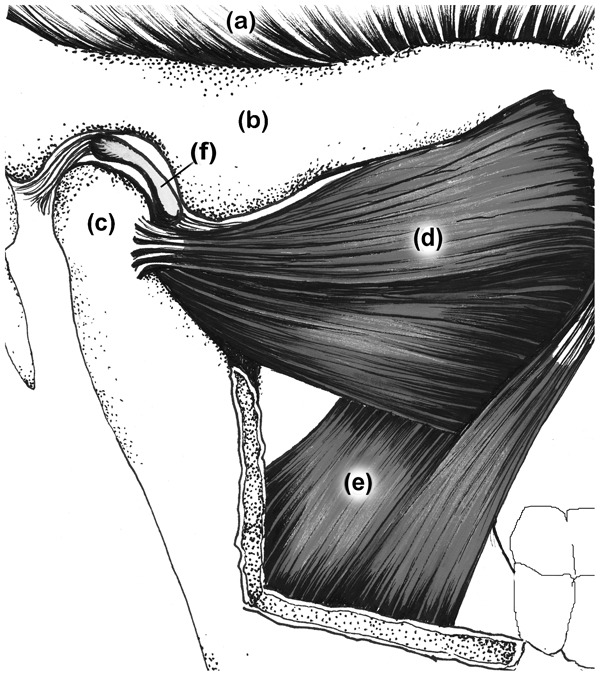
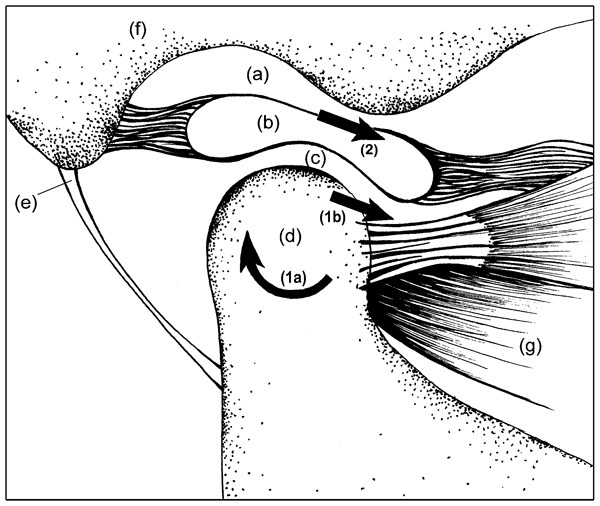
Temporomandibular disorders (TMD) are a heterogeneous group of diagnoses affecting the temporomandibular joint (TMJ) and surrounding tissues. A variety of methods for evaluating and managing TMD have been proposed within the physical therapy profession but these sources are not peer-reviewed and lack updates from scientific literature. The dental profession has provided peer-reviewed sources that lack thoroughness with respect to the neuromusculoskeletal techniques utilized by physical therapists. The subsequent void creates the need for a thorough, research informed, and peer-reviewed source regarding TMD evaluation and management for physical therapists. This paper is the first part in a two-part series that seeks to fill the current void by providing a brief but comprehensive outline for clinicians seeking to provide services for patients with TMD. Part one focuses on anatomy and pathology, arthro- and osteokinematics, epidemiology, history taking, and physical examination as they relate to TMD. An appreciation of the anatomical and mechanical features associated with the TMJ can serve as a foundation for understanding a patient's clinical presentation. Performance of a thorough patient history and clinical examination can guide the clinician toward an improved diagnostic process.
Keywords: Diagnosis; Physical examination; Review; Temporomandibular joint disorders.
Figures
References
-
- McNeill C. History and evolution of TMD concepts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:51–60. - PubMed
-
- Griffiths RH. Report of the president’s conference on the examination, diagnosis, and management of temporomandibular disorders. J Am Dent Assoc. 1983;106:75–7. - PubMed
-
- Winkel D, Aufdemkampe G, Matthijs O, Meijer OG, Phelps V.Temporomandibular joint. Diagnosis and treatment of the spine: nonoperative orthopaedic medicine and manual therapy Gaithersburg: Aspen Publishers; 1996. p. 715–68.
-
- Widmer CG.Evaluation of temporomandibular disorders In: Krause SL, editor. TMJ disorders, management of the craniomandibular complexNew York, NY, USA: Churchill Livingstone; 1988. p. 79–112.
-
- Kaltenborn FM, Evjenth O, Baldauf Kaltenborn T, Morgan D, Vollowitz E. 2003. Manual mobilization of the joints: volume 2, the spine, 4th edn. Oslo.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical