

Temporomandibular disorders. Part 2: conservative management
- PMID: 24976744
- PMCID: PMC4062348
- DOI: 10.1179/2042618613Y.0000000061
Temporomandibular disorders. Part 2: conservative management
Abstract
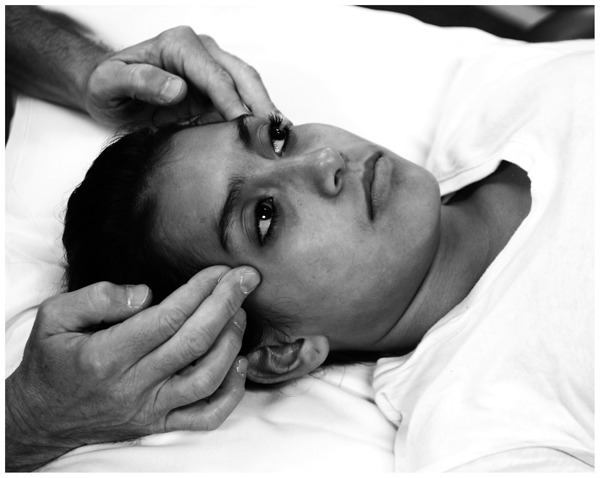
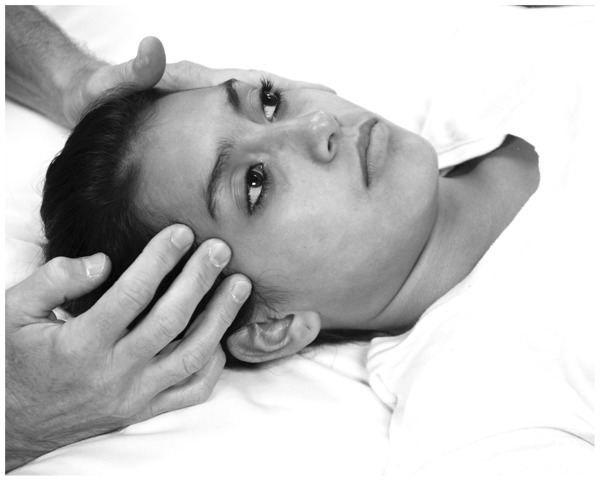
Appropriate management of temporomandibular disorders (TMD) requires an understanding of the underlying dysfunction associated with the temporomandibular joint (TMJ) and surrounding structures. A comprehensive examination process, as described in part 1 of this series, can reveal underlying clinical findings that assist in the delivery of comprehensive physical therapy services for patients with TMD. Part 2 of this series focuses on management strategies for TMD. Physical therapy is the preferred conservative management approach for TMD. Physical therapists are professionally well-positioned to step into the void and provide clinical services for patients with TMD. Clinicians should utilize examination findings to design rehabilitation programs that focus on addressing patient-specific impairments. Potentially appropriate plan of care components include joint and soft tissue mobilization, trigger point dry needling, friction massage, therapeutic exercise, patient education, modalities, and outside referral. Management options should address both symptom reduction and oral function. Satisfactory results can often be achieved when management focuses on patient-specific clinical variables.
Keywords: Conservative management; Review; Temporomandibular joint disorders.
Figures






References
-
- Young B, Walker MJ, Strunce J, Boyles R. A combined treatment approach emphasizing impairment-based manual physical therapy for plantar heel pain: a case series. J Orthop Sports Phys Ther. 2004;34:725–33. - PubMed
-
- Furto ES, Cleland JA, Whitman JM, Olson KA. Manual physical therapy interventions and exercise for patients with temporomandibular disorders. Cranio. 2006;24:283–91. - PubMed
-
- Walker MJ, Boyles RE, Young BA, Strunce JB, Garber MB, Whitman JM, et al. The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial. Spine. 2008;33:2371–8. - PubMed
-
- List T, Axelsson S. Management of TMD: evidence from systematic reviews and meta-analyses. J Oral Rehabil. 2010;37:430–51. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical