

Osteosarcoma in pediatric patients and young adults: a single institution retrospective review of presentation, therapy, and outcome
- PMID: 24976784
- PMCID: PMC4021746
- DOI: 10.1155/2014/402509
Osteosarcoma in pediatric patients and young adults: a single institution retrospective review of presentation, therapy, and outcome
Abstract
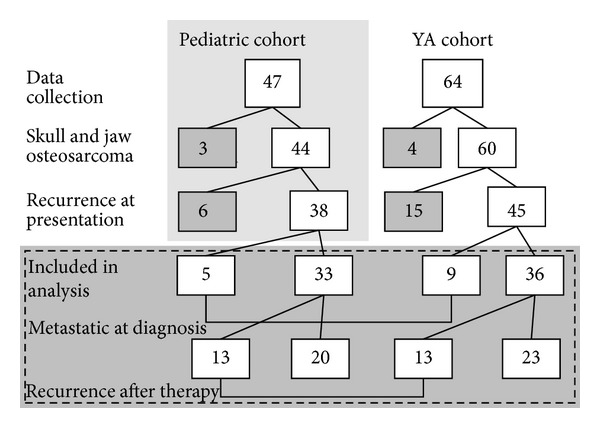
Background. Little is known about how cumulative chemotherapy delivery influences the poorer outcome observed in young adult (YA, 18-40 years) versus pediatric (<18 years) osteosarcoma patients. Here, we retrospectively examined differences in presentation, therapy, including cumulative chemotherapy dose, and outcome in YA and pediatric patients. Methods. We reviewed 111 cases of high-grade osteosarcoma at Moffitt Cancer Center between 1988 and 2012. Presentation factors, therapies, and survival were compared between YA and pediatric cohorts. Results. The cohorts were equivalent with respect to metastatic status, gender, tumor size, tumor site, and histological subtype. We found that the YA patients tended to have poorer histologic response to neoadjuvant chemotherapy measured by necrosis with 55% and 35% of pediatric versus YA patients responding favorably (P = 0.06). Only 39% of YA patients achieved the typical pediatric dose of methotrexate, doxorubicin, and cisplatin. These patients had a 3-year EFS of 76% (CI 53-100%) versus 47% (CI 26-69%; P = 0.09) in those who received less chemotherapy. Conclusion. Age continues to be a prognostic factor in osteosarcoma. Our study suggests that presentation factors are not associated with prognosis, while poorer response to chemotherapy and lower cumulative dose of chemotherapy delivered to YA patients may contribute to poorer outcomes.
Figures


References
-
- Friedman MA, Carter SK. The therapy of osteogenic sarcoma: current status and thoughts for the future. Journal of Surgical Oncology. 1972;4(5):482–510. - PubMed
-
- Bernthal NM, Federman N, Eilber FR, et al. Long-term results (>25 years) of a randomized, prospective clinical trial evaluating chemotherapy in patients with high-grade, operable osteosarcoma. Cancer. 2012;118(23):5888–5893. - PubMed
-
- Meyers PA, Gorlick R, Heller G, et al. Intensification of preoperative chemotherapy for osteogenic sarcoma: results of the Memorial Sloan-Kettering (T12) protocol. Journal of Clinical Oncology. 1998;16(7):2452–2458. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
