

Multi-detector computed tomography in the diagnosis and management of acute aortic syndromes
- PMID: 24976936
- PMCID: PMC4072820
- DOI: 10.4329/wjr.v6.i6.355
Multi-detector computed tomography in the diagnosis and management of acute aortic syndromes
Abstract
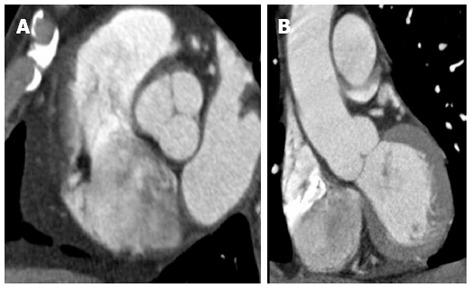
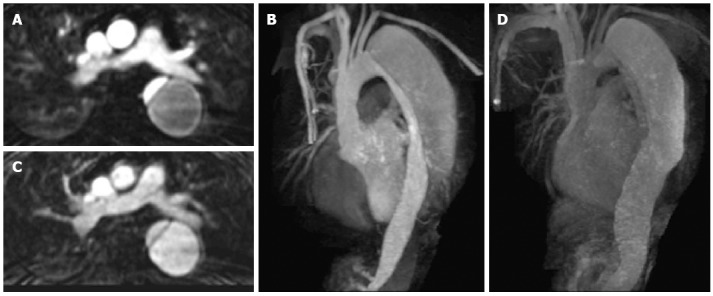
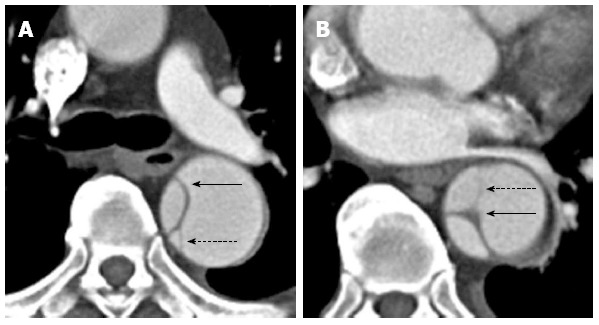
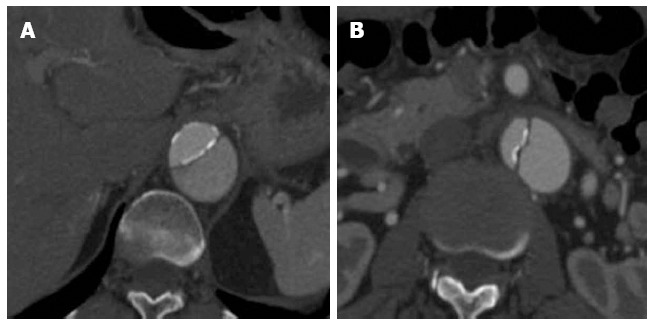
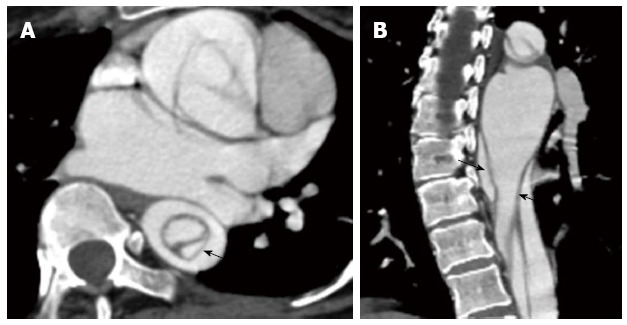
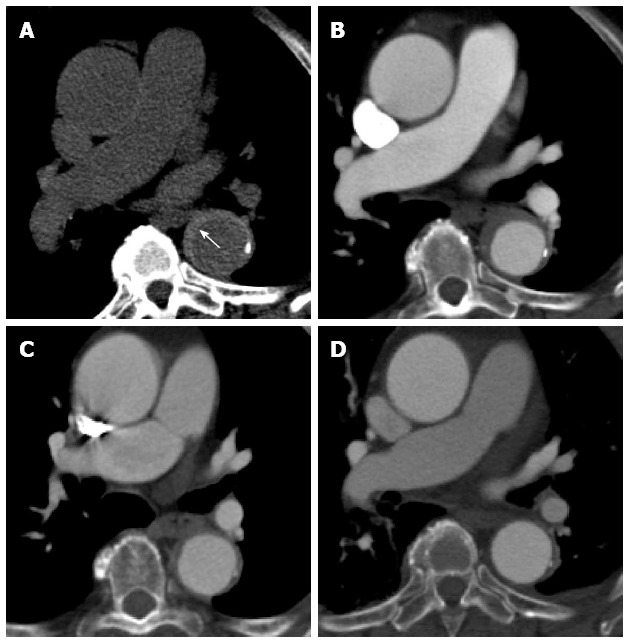
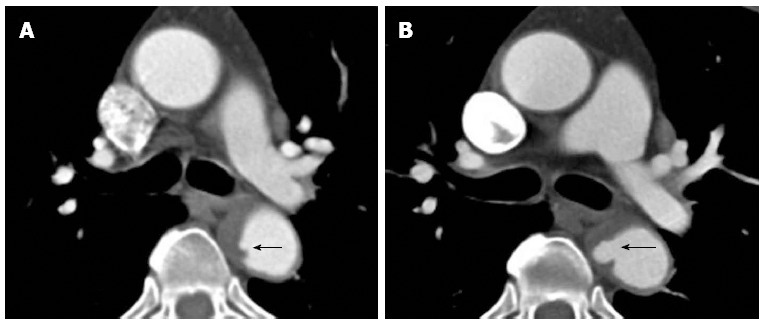
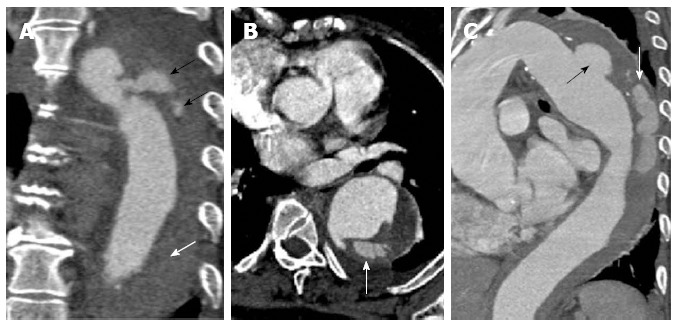
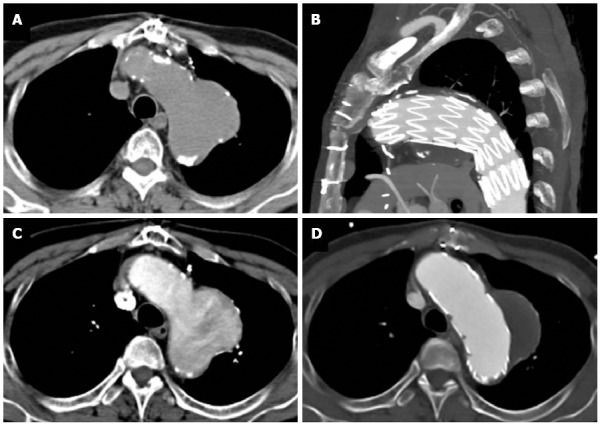
Acute aortic syndrome (AAS) is a spectrum of conditions, which may ultimately progress to potentially life-threatening aortic rupture. This syndrome encompasses aortic dissection (AD), intramural haematoma, penetrating atherosclerotic ulcer and unstable thoracic aortic aneurysms. Multi-detector CT (MDCT) is crucial for the diagnosis of AAS, especially in the emergency setting due to its speed, accuracy and ready availability. This review attends to the value of appropriate imaging protocols in obtaining good quality images that can permit a confident diagnosis of AAS. AD is the most commonly encountered AAS and also the one with maximum potential to cause catastrophic outcome if not diagnosed and managed promptly. Hence, this review briefly addresses certain relevant clinical perspectives on this condition. Differentiating the false from the true lumen in AD is often essential; a spectrum of CT findings, e.g., "beak sign", aortic "cobwebs" that allows such differentiation have been described with explicit illustrations. The value of non enhanced CT scans, especially useful in the diagnosis of an intramural hematoma has also been illustrated. Overlap in the clinical and imaging features of the various conditions presenting as AAS is not unusual. However, on most instances MDCT enables the right diagnosis. On select occasions MRI or trans-esophageal echocardiography may be required as a problem solving tool.
Keywords: Acute aortic syndrome; Aortic aneurysm; Aortic dissection; Computed tomography scan; Intramural haematoma; Penetrating aortic ulcer.
Figures


References
-
- Chiu KW, Lakshminarayan R, Ettles DF. Acute aortic syndrome: CT findings. Clin Radiol. 2013;68:741–748. - PubMed
-
- Nienaber CA, Powell JT. Management of acute aortic syndromes. Eur Heart J. 2012;33:26–35b. - PubMed
-
- Jánosi RA, Erbel R, Konorza TF. Recent advances in the diagnosis of acute aortic syndromes. Expert Opin Med Diagn. 2012;6:529–540. - PubMed
-
- Akin I, Kische S, Ince H, Nienaber C. Penetrating aortic ulcer, intramural hematoma, acute aortic syndrome: when to do what. J Cardiovasc Surg (Torino) 2012;53:83–90. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
