

The epidemiology and demographics of hip dysplasia
- PMID: 24977057
- PMCID: PMC4063216
- DOI: 10.5402/2011/238607
The epidemiology and demographics of hip dysplasia
Abstract
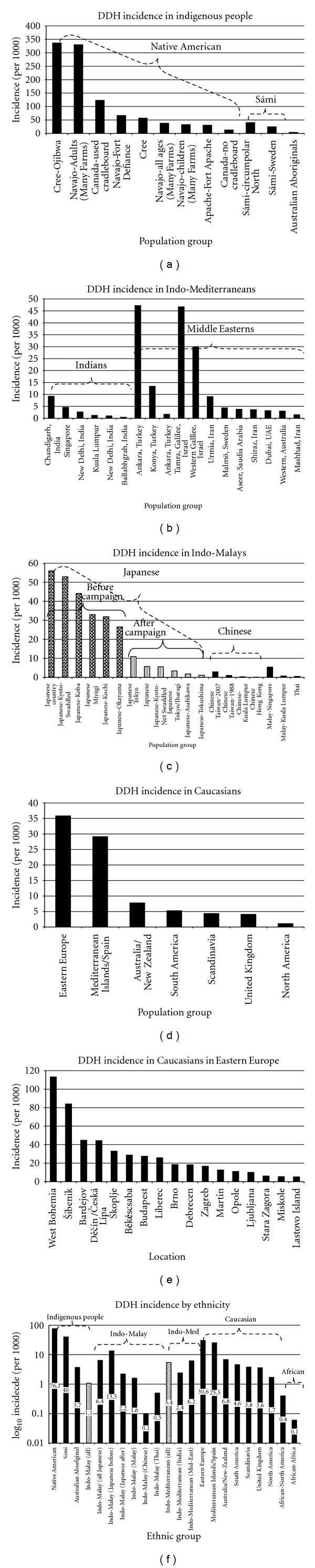
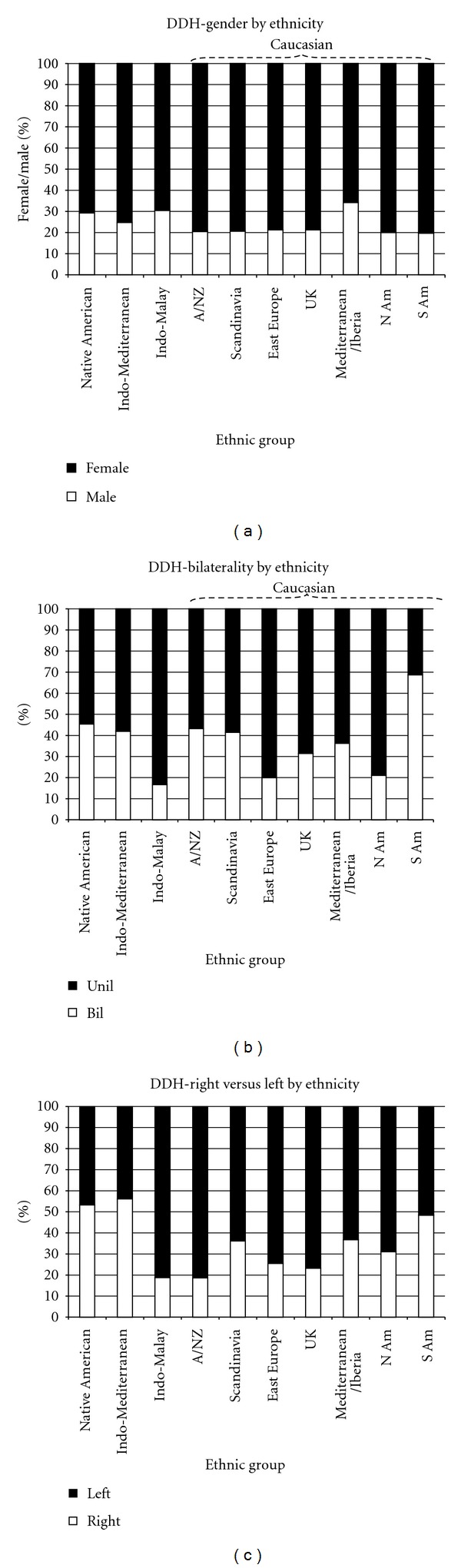
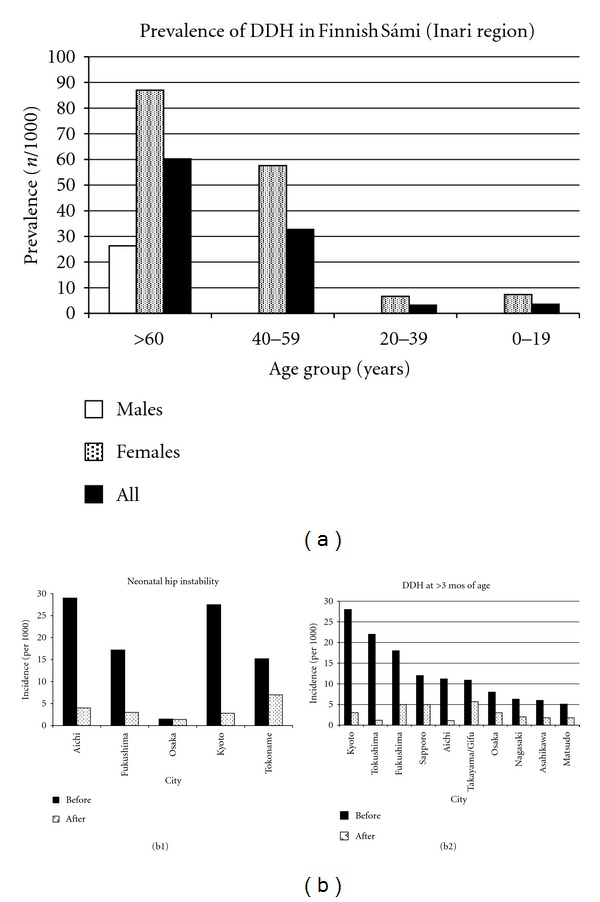
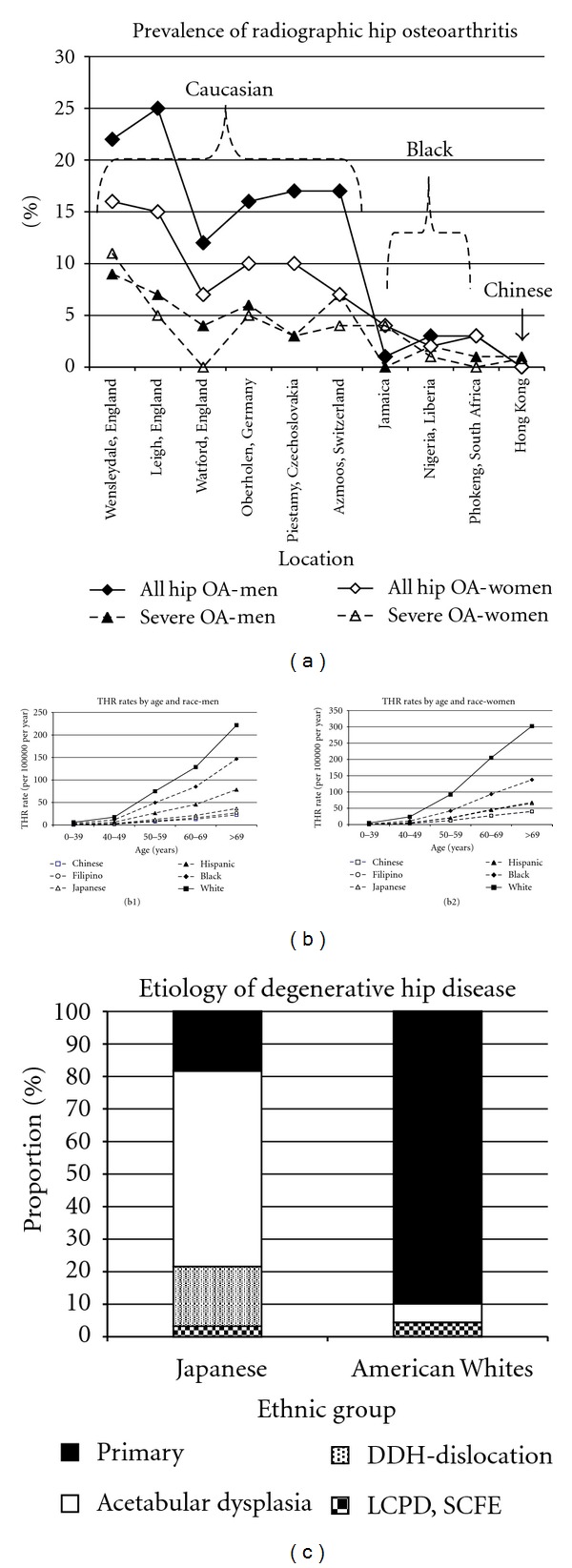
The etiology of developmental dysplasia of the hip (DDH) is unknown. There are many insights, however, from epidemiologic/demographic information. A systematic medical literature review regarding DDH was performed. There is a predominance of left-sided (64.0%) and unilateral disease (63.4%). The incidence per 1000 live births ranges from 0.06 in Africans in Africa to 76.1 in Native Americans. There is significant variability in incidence within each racial group by geographic location. The incidence of clinical neonatal hip instability at birth ranges from 0.4 in Africans to 61.7 in Polish Caucasians. Predictors of DDH are breech presentation, positive family history, and gender (female). Children born premature, with low birth weights, or to multifetal pregnancies are somewhat protected from DDH. Certain HLA A, B, and D types demonstrate an increase in DDH. Chromosome 17q21 is strongly associated with DDH. Ligamentous laxity and abnormalities in collagen metabolism, estrogen metabolism, and pregnancy-associated pelvic instability are well-described associations with DDH. Many studies demonstrate an increase of DDH in the winter, both in the northern and southern hemispheres. Swaddling is strongly associated with DDH. Amniocentesis, premature labor, and massive radiation exposure may increase the risk of DDH. Associated conditions are congenital muscular torticollis and congenital foot deformities. The opposite hip is frequently abnormal when using rigorous radiographic assessments. The role of acetabular dysplasia and adult hip osteoarthritis is complex. Archeological studies demonstrate that the epidemiology of DDH may be changing.
Figures
References
-
- Stedman TL. Stedman’s Medical Dictionary. 26th edition. Baltimore, Md, USA: Williams and Wilkins; 1995.
-
- Kocher MS, Zurakowski D. Clinical epidemiology and biostatistics: a primer for orthopaedic surgeons. Journal of Bone and Joint Surgery, American. 2004;86(3):607–620. - PubMed
-
- Szabo RM. Principles of epidemiology for the orthopaedic surgeon. Journal of Bone and Joint Surgery, American. 1998;80(1):111–120. - PubMed
-
- MacFarlane A. Congenital dislocation of the hip—an epidemiological conunmdrum. Maternal and Child Health Journal. 1980:13–15.
-
- Homer CJ, Baltz RD, Hickson GB, et al. Clinical practice guideline: early detection of developmental dysplasia of the hip. Pediatrics. 2000;105(4 I):896–905. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials