

Osteoporosis and fractures in HIV/hepatitis C virus coinfection: a systematic review and meta-analysis
- PMID: 24977441
- PMCID: PMC4940983
- DOI: 10.1097/QAD.0000000000000363
Osteoporosis and fractures in HIV/hepatitis C virus coinfection: a systematic review and meta-analysis
Abstract
Objective: There is growing evidence that fracture risk is increased in individuals with HIV and/or hepatitis C virus (HCV) infection. We systematically reviewed the literature to determine whether prevalence of osteoporosis and incidence of fracture is increased in HIV/HCV-coinfected individuals.
Design: A systematic review and meta-analysis.
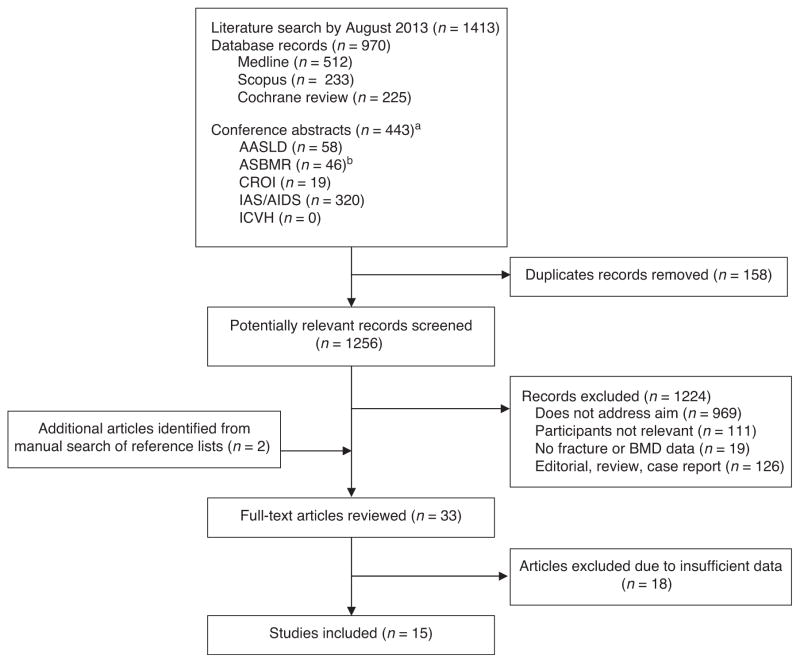
Methods: A search was performed of Medline, Scopus and the Cochrane Library databases, as well as of abstracts from annual retroviral, liver and bone meetings (up to 2013) for studies with bone mineral density (BMD) or bone fracture data for HIV/ HCV-coinfected individuals. Osteoporosis odds ratios (ORs) and fracture incidence rate ratios (IRRs) were estimated from studies with data on HIV-monoinfected or HIV/HCV uninfected comparison groups.
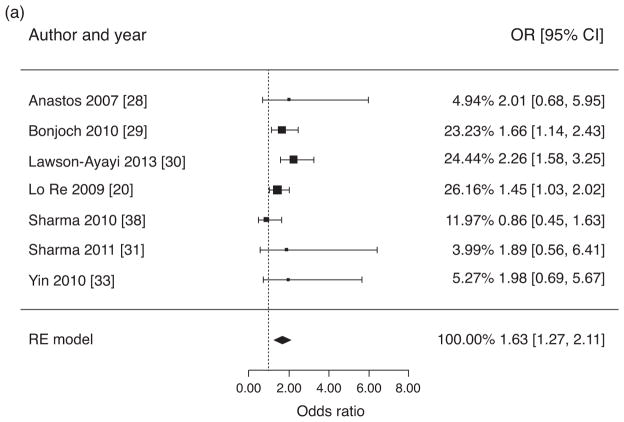
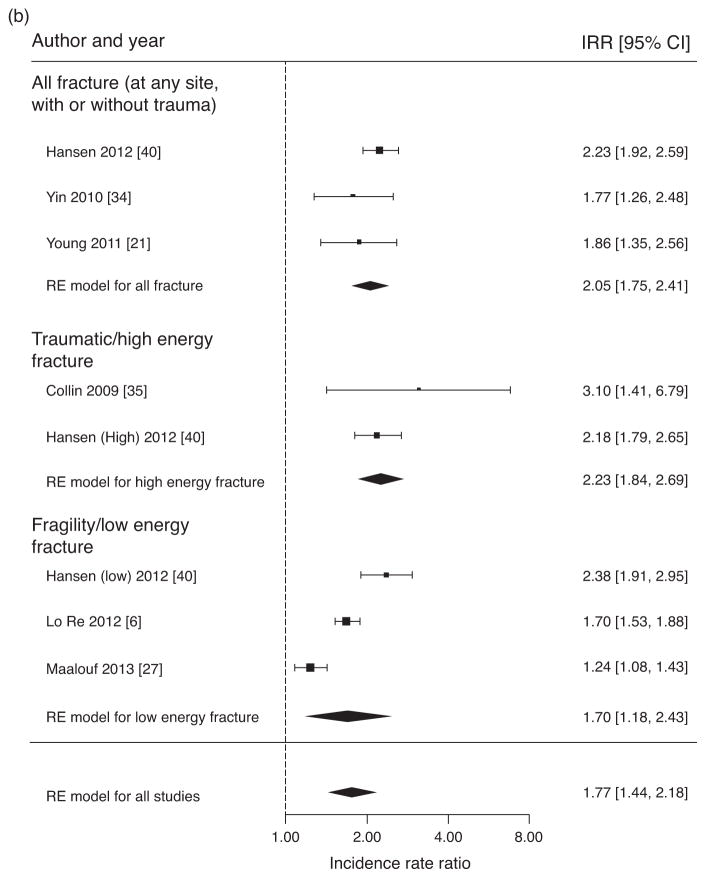
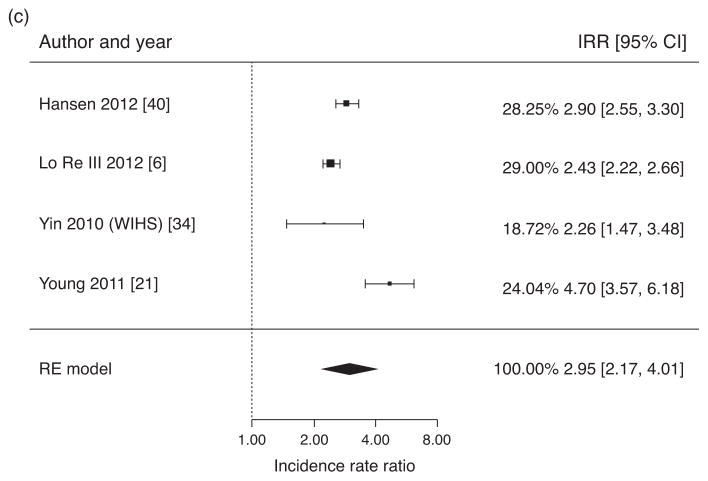
Results: Of 15 included studies, nine reported BMD data and six reported fracture data. For HIV/HCV-coinfected, the estimated osteoporosis prevalence was 22% [95% confidence interval (95% CI) 12–31] and the crude OR for osteoporosis compared with HIV-monoinfected was 1.63 (95% CI 1.27-2.11). The pooled IRR of overall fracture risk for HIV/HCV-coinfected individuals was 1.77 (95% CI 1.44-2.18) compared with HIV-monoinfected and 2.95 (95% CI 2.17-4.01) compared with uninfected individuals. In addition to HIV/HCV-coinfection, older age, lower BMI, smoking, alcohol and substance use were significant predictors of osteoporosis and fractures across studies.
Conclusion: HIV/HCV coinfection is associated with a greater risk of osteoporosis and fracture than HIV monoinfection; fracture risk is even greater than uninfected controls. These data suggest that HIV/HCV-coinfected individuals should be targeted for fracture prevention through risk factor modification at all ages and DXA screening at age 50.
Conflict of interest statement
M.T.Y. has served as a consultant for Gilead and Abbvie.
The other authors have no conflicts of interest.
Figures
Similar articles
-
Effectiveness and safety of vitamin D in relation to bone health.Evid Rep Technol Assess (Full Rep). 2007 Aug;(158):1-235. Evid Rep Technol Assess (Full Rep). 2007. PMID: 18088161 Free PMC article.
-
Vitamin D and vitamin D analogues for preventing fractures in post-menopausal women and older men.Cochrane Database Syst Rev. 2014 Apr 14;2014(4):CD000227. doi: 10.1002/14651858.CD000227.pub4. Cochrane Database Syst Rev. 2014. PMID: 24729336 Free PMC article.
-
Calcium and vitamin D for increasing bone mineral density in premenopausal women.Cochrane Database Syst Rev. 2023 Jan 27;1(1):CD012664. doi: 10.1002/14651858.CD012664.pub2. Cochrane Database Syst Rev. 2023. PMID: 36705288 Free PMC article.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.Health Technol Assess. 2008 Mar;12(3):iii-ix, xi-xiv, 1-208. doi: 10.3310/hta12030. Health Technol Assess. 2008. PMID: 18284894
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.Health Technol Assess. 2005 Jun;9(22):1-160. doi: 10.3310/hta9220. Health Technol Assess. 2005. PMID: 15929857
Cited by
-
Association of Respiratory Tuberculosis with Incident Bone Fracture: Bridging the Tuberculosis Airway Infection and the Osteoporotic Bone.PLoS One. 2016 Dec 22;11(12):e0168673. doi: 10.1371/journal.pone.0168673. eCollection 2016. PLoS One. 2016. PMID: 28005963 Free PMC article.
-
HIV and Bone Complications: Understudied Populations and New Management Strategies.Curr HIV/AIDS Rep. 2016 Dec;13(6):349-358. doi: 10.1007/s11904-016-0341-9. Curr HIV/AIDS Rep. 2016. PMID: 27730445 Review.
-
A case-control study based on the National Health and Nutrition Examination Survey to evaluate the effects of human papilloma virus on bone health in women.BMC Med. 2025 Feb 7;23(1):75. doi: 10.1186/s12916-025-03909-2. BMC Med. 2025. PMID: 39920637 Free PMC article.
-
Brief communication: comorbidities and aging in people living with HIV.AIDS Res Ther. 2024 Oct 26;21(1):77. doi: 10.1186/s12981-024-00667-8. AIDS Res Ther. 2024. PMID: 39462421 Free PMC article. Review.
-
Usefulness of calcaneal quantitative ultrasound stiffness for the evaluation of bone health in HIV-1-infected subjects: comparison with dual X-ray absorptiometry.HIV AIDS (Auckl). 2016 May 31;8:109-17. doi: 10.2147/HIV.S99904. eCollection 2016. HIV AIDS (Auckl). 2016. PMID: 27330330 Free PMC article.
References
-
- Mitchell AE, Colvin HM, Palmer Beasley R. Institute of Medicine recommendations for the prevention and control of hepatitis B and C. Hepatology. 2010;51:729–733. - PubMed
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57:1333–1342. - PubMed
-
- Loria I, Albanese C, Giusto M, Galtieri PA, Giannelli V, Lucidi C, et al. Bone disorders in patients with chronic liver disease awaiting liver transplantation. Transplant Proc. 2010;42:1191–1193. - PubMed
-
- Carey EJ, Balan V, Kremers WK, Hay JE. Osteopenia and osteoporosis in patients with end-stage liver disease caused by hepatitis C and alcoholic liver disease: not just a cholestatic problem. Liver Transplant. 2003;9:1166–1173. - PubMed
-
- Lin JC, Hsieh TY, Wu CC, Chen PJ, Chueh TH, Chang WK, et al. Association between chronic hepatitis C virus infection and bone mineral density. Calcif Tissue Int. 2012;91:423–429. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
