

2013 Dade W. Moeller lecture: medical countermeasures against radiological terrorism
- PMID: 24978287
- PMCID: PMC4076685
- DOI: 10.1097/HP.0000000000000082
2013 Dade W. Moeller lecture: medical countermeasures against radiological terrorism
Abstract
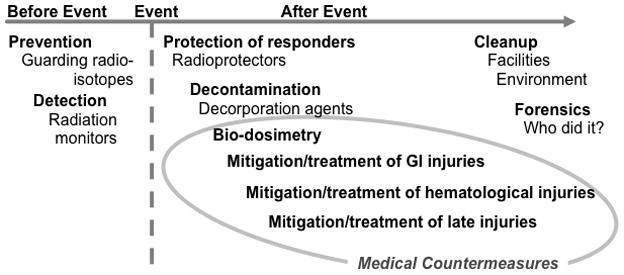
Soon after the 9-11 attacks, politicians and scientists began to question our ability to cope with a large-scale radiological terrorism incident. The outline of what was needed was fairly obvious: the ability to prevent such an attack, methods to cope with the medical consequences, the ability to clean up afterward, and the tools to figure out who perpetrated the attack and bring them to justice. The medical response needed three components: the technology to determine rapidly the radiation doses received by a large number of people, methods for alleviating acute hematological radiation injuries, and therapies for mitigation and treatment of chronic radiation injuries. Research done to date has shown that a realistic medical response plan is scientifically possible, but the regulatory and financial barriers to achieving this may currently be insurmountable.
Figures

References
-
- Acevedo SF, McGinnis G, Raber J. Effects of 137Cs γ irradiation on cognitive performance and measures of anxiety in Apoe−/− and wild-type female mice. Radiat Res. 2008;170:422–428. - PubMed
-
- Anno GH, McClellan GE, Dore MA. Protracted radiation-induced performance decrement. Volume 1: Model development. Santa Monica, United States: Pacific-Sierra Research Corporation; 1995.
-
- Anno GH, Young RW, Bloom RM, Mercier JR. Dose response relationships for acute ionizing-radiation lethality. Health Phys. 2003;84:565–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
