

Treatment of advanced Parkinson's disease
- PMID: 24978634
- PMCID: PMC4140171
- DOI: 10.1097/WCO.0000000000000118
Treatment of advanced Parkinson's disease
Abstract
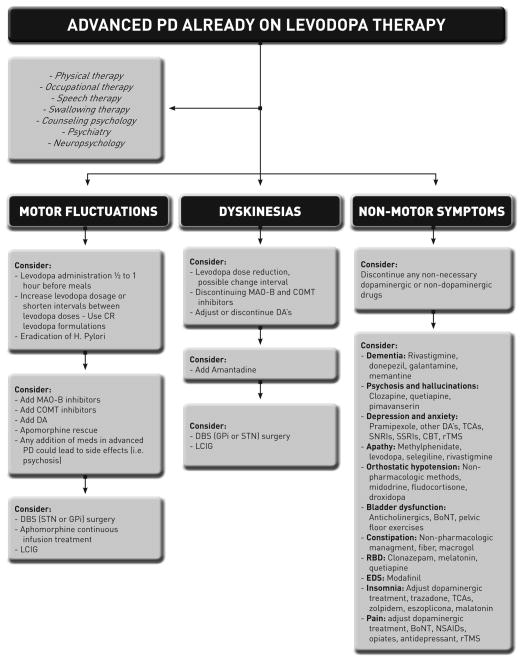
Purpose of review: Later stage Parkinson's disease, sometimes referred to as advanced disease, has been characterized by motor complication, as well as by the potential emergence of nonlevodopa responsive motor and nonmotor symptoms. The management of advanced stage Parkinson's disease can be complex. This review summarizes the currently available treatment strategies for addressing advanced Parkinson's disease.
Recent findings: We will discuss the latest pharmacological strategies (e.g., inhibitors of dopamine-metabolizing enzymes, dopamine agonists, and extended release dopamine formulations) for addressing motor dysfunction. We will summarize the risks and benefits of current invasive treatments. Finally, we will address the current evidence supporting the treatment of nonmotor symptoms in the advanced Parkinson's disease patient. We will conclude by detailing the potential nonpharmacological and multidisciplinary approaches for advanced stage Parkinson's disease.
Summary: The optimization of levodopa is, in most cases, the most powerful therapeutic option available; however, medication optimization requires an advanced understanding of Parkinson's disease. Failure of conventional pharmacotherapy should precipitate a discussion of the potential risks and benefits of more invasive treatments. Currently, there are no comparative studies of invasive treatment. Among the invasive treatments, deep brain stimulation has the largest amount of existing evidence, but also has the highest individual per patient risk. Nonmotor symptoms will affect quality of life more than the motor Parkinson's disease symptoms, and these nonmotor symptoms should be aggressively treated. Many advanced Parkinson's disease patients will likely benefit from multi and interdisciplinary Parkinson's disease teams with multiple professionals collaborating to develop a collective and tailored strategy for an individual patient.
Conflict of interest statement
Dr. Giugni: none declared
Dr. Okun: serves as a consultant for the National Parkinson Foundation, and has received research grants from NIH, NPF, the Michael J. Fox Foundation, the Parkinson Alliance, Smallwood Foundation, the Bachmann-Strauss Foundation, the Tourette Syndrome Association, and the UF Foundation. Dr. Okun has previously received honoraria, but in the past >48 months has received no support from industry. Dr. Okun has received royalties for publications with Demos, Manson, Amazon, Smashwords, and Cambridge (movement disorders books). Dr. Okun is an associate editor for New England Journal of Medicine Journal Watch Neurology. Dr. Okun has participated in CME activities on movement disorders (in the last 36) months sponsored by PeerView, Prime, and by Vanderbilt University. The institution and not Dr. Okun receives grants from Medtronic and ANS/St. Jude, and the PI has no financial interest in these grants. Dr. Okun has participated as a site PI and/or co-I for several NIH, foundation, and industry sponsored trials over the years but has not received honoraria.
Figures
References
-
- Shulman LM, Gruber-Baldini AL, Anderson KE, et al. The evolution of disability in Parkinson disease. Movement disorders: official journal of the Movement Disorder Society. 2008;23(6):790–6. - PubMed
-
- Hauser RA, McDermott MP, Messing S. Factors associated with the development of motor fluctuations and dyskinesias in Parkinson disease. Archives of neurology. 2006;63(12):1756–60. - PubMed
-
- Hely MA, Morris JG, Reid WG, Trafficante R. Sydney Multicenter Study of Parkinson’s disease: non-L-dopa-responsive problems dominate at 15 years. Movement disorders: official journal of the Movement Disorder Society. 2005;20(2):190–9. - PubMed
-
- Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. 1967;17(5):427–42. - PubMed
-
- Hoehn MM. Parkinsonism treated with levodopa: progression and mortality. Journal of neural transmission Supplementum. 1983;19:253–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
