

Unexpected post-operative diagnosis of primary rectal melanoma. A case report
- PMID: 24979106
- PMCID: PMC4321517
Unexpected post-operative diagnosis of primary rectal melanoma. A case report
Abstract
Aim: Anorectal melanoma (ARM) is a very uncommon and highly lethal malignancy. Due to its rarity and non-specific symptoms, preoperative diagnosis may be often erroneous and subsequent treatment inappropriate. We report a case of primary rectal melanoma and discuss the current diagnostic and therapeutic challenges.
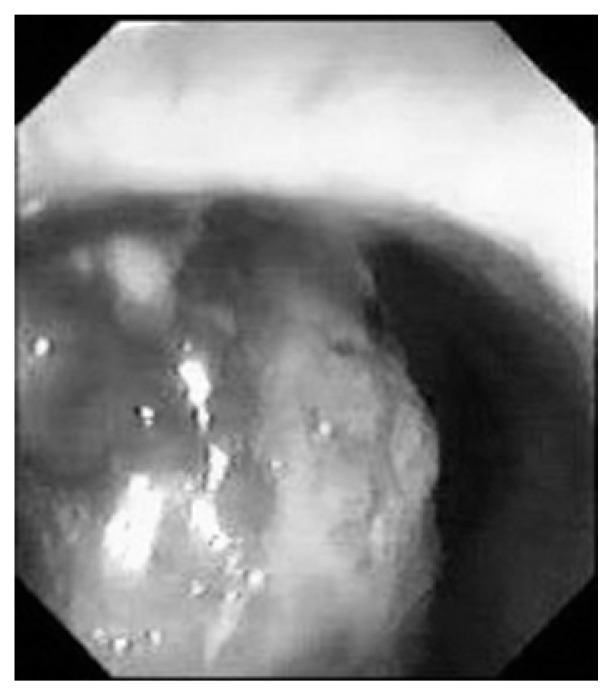
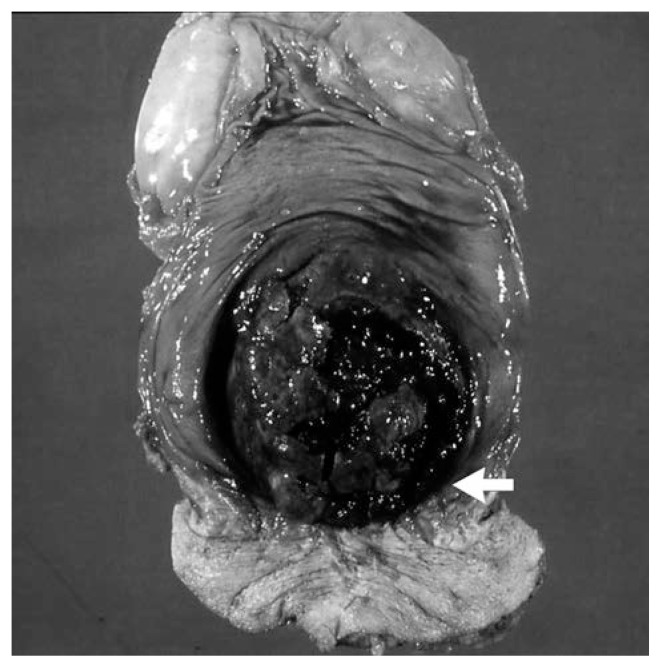
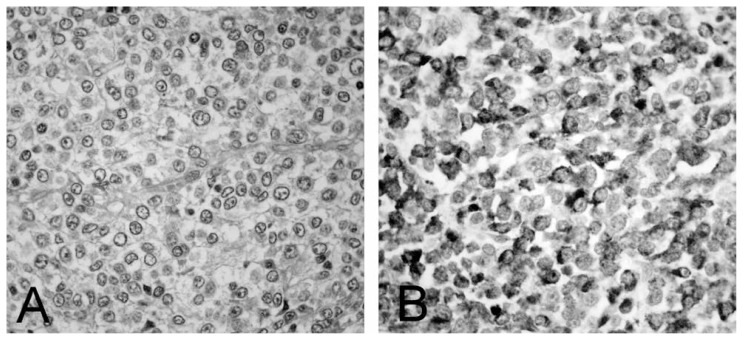
Case report: An 87-year-old man was admitted to our surgical unit with a history of progressive constipation, tenesmus, rectal bleeding and transanal mucous discharge. Preoperative investigations, including CT scan and colonoscopy with biopsy, were suggestive for locally advanced low rectal sarcoma and therefore the patient underwent abdominoperineal resection (APR). However, histopathological examination and immunohistochemistry resulted in a postoperative diagnosis of primary rectal melanoma. The patient died 6 months later due to local and systemic recurrence.
Conclusion: ARM should always be considered when unusual anorectal lesions are discovered. Regardless of the pathological stage and the extent of surgery, prognosis of ARM remains poor. Thus, whenever feasible, wide local excision is now the preferred treatment, since it is associated with lower postoperative morbidity and better quality of life compared to APR. In our case, although the initial diagnosis was incorrect, APR was justified by the local invasiveness and large size of the tumor.
Figures
References
-
- Meguerditchian AN, Meterissian SH, Dunn KB. Anorectal melanoma: diagnosis and treatment. Dis Colon Rectum. 2011;54:638–44. - PubMed
-
- Yap LB, Neary P. A comparison of wide local excision with abdominoperineal resection in anorectal melanoma. Melanoma research. 2004;14:147–150. - PubMed
-
- Falch C, Stojadinovic A, Hannvon-Weyhern C, Protic M, Nissan A, Faries MB, Daumer M, Bilchik AJ, Itzhak A, Brücher BL. Anorectal malignant melanoma: extensive 45-year review and proposal for a novel staging classification. J Am Coll Surg. 2013;217:324–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous