

Pancreatectomy predicts improved survival for pancreatic adenocarcinoma: results of an instrumental variable analysis
- PMID: 24979599
- PMCID: PMC4277740
- DOI: 10.1097/SLA.0000000000000796
Pancreatectomy predicts improved survival for pancreatic adenocarcinoma: results of an instrumental variable analysis
Abstract
Background and objective: Pancreatic resection is the standard treatment option for patients with stage I/II pancreatic ductal adenocarcinoma (PDA), yet many studies demonstrate low rates of resection. The objective of this study was to evaluate whether increasing resection rates would result in an increase in average survival in patients with stage I/II PDA.
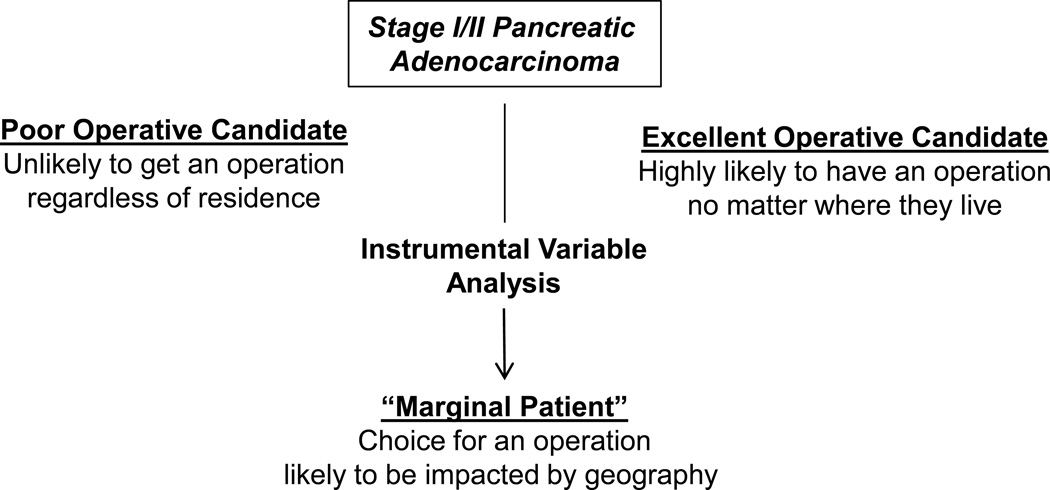
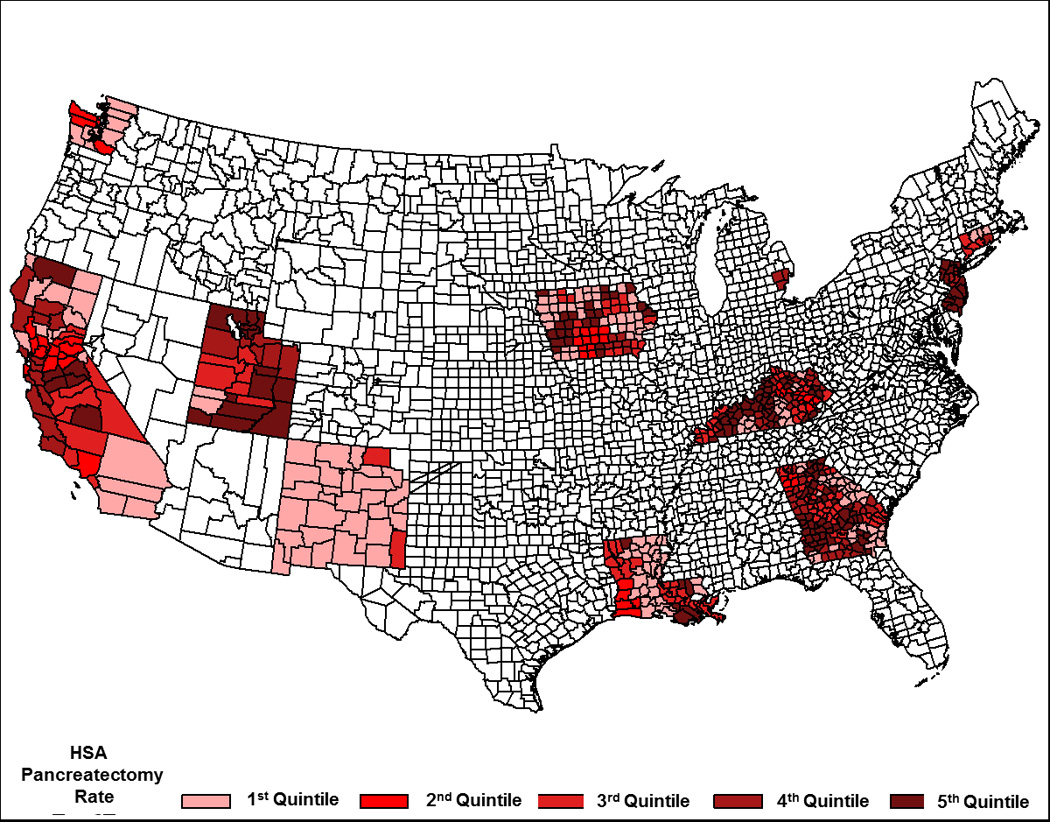
Methods: SEER (Surveillance, Epidemiology, and End Results) data were analyzed for patients with stage I/II pancreatic head cancers treated from 2004 to 2009. Pancreatectomy rates were examined within Health Service Areas (HSAs) across 18 SEER regions. An instrumental variable analysis was performed, using HSA rates as an instrument, to determine the impact of increasing resection rates on survival.
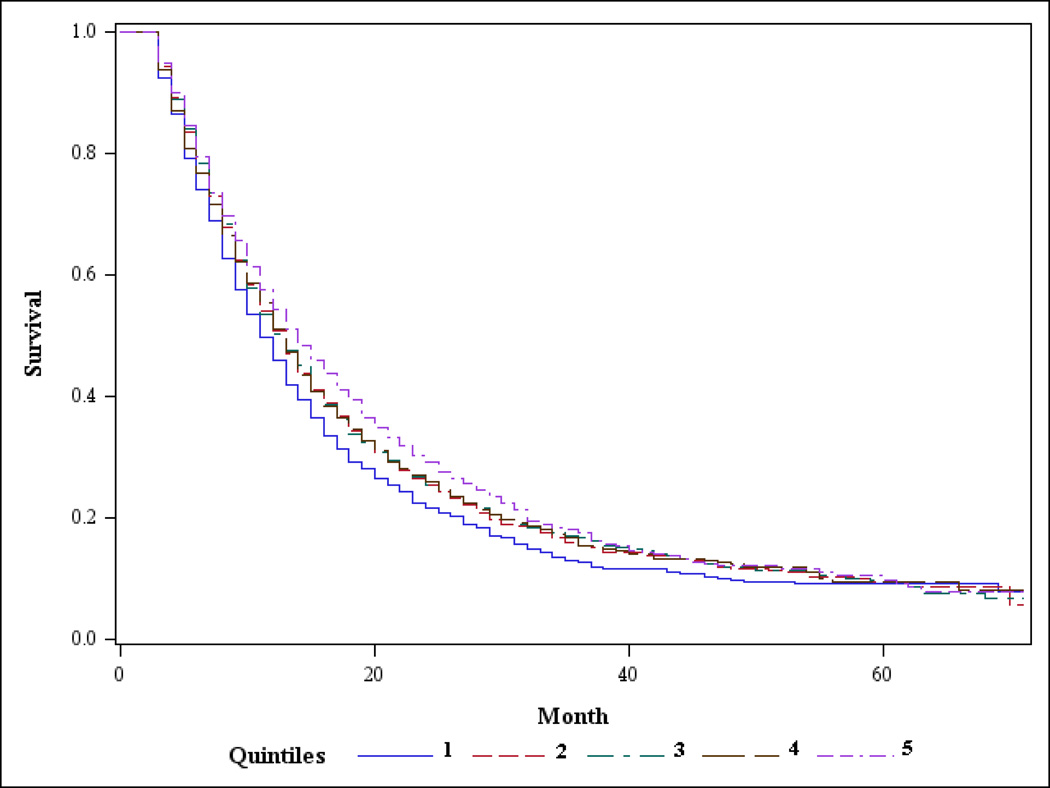
Results: Pancreatectomy was performed in 4322 of 8323 patients evaluated with stage I/II PDA (overall resection rate = 51.9%). The resection rate across HSAs ranged from an average of 38.6% (lowest quintile) to 67.3% (highest quintile). Median survival was improved in HSAs with higher resection rates. Instrumental variable analysis revealed that, for patients whose treatment choices were influenced by rates of resection in their geographic region, pancreatectomy was associated with a statistically significant increase in overall survival.
Conclusions: When controlling for confounders using instrumental variable analysis, pancreatectomy is associated with a statistically significant increase in survival for patients with resectable PDA. On the basis of these results, if resection rates were to increase in select patients, then average survival would also be expected to increase. It is important that this information be provided to physicians and patients so that they can properly weigh the risks and advantages of pancreatectomy as treatment of PDA.
Conflict of interest statement
The authors have no financial disclosures or conflicts of interest.
Figures
References
-
- Li D, Xie K, Wolff R, et al. Pancreatic cancer. Lancet. 2004 Mar 27;363(9414):1049. - PubMed
-
- Baxter NN, Whitson BA, Tuttle TM. Trends in the treatment and outcome of pancreatic cancer in the United States. Ann.Surg.Oncol. 2007 Apr;14(4):1320. - PubMed
-
- Konstantinidis IT, Warshaw AL, Allen JN, et al. Pancreatic ductal adenocarcinoma: is there a survival difference for R1 resections versus locally advanced unresectable tumors? What is a "true" R0 resection? Annals of surgery. 2013 Apr;257(4):731–736. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
