

Diagnostic imaging modalities in head and neck disease
- PMID: 24980674
- PMCID: PMC4078224
- DOI: 10.3238/arztebl.2014.0417
Diagnostic imaging modalities in head and neck disease
Abstract
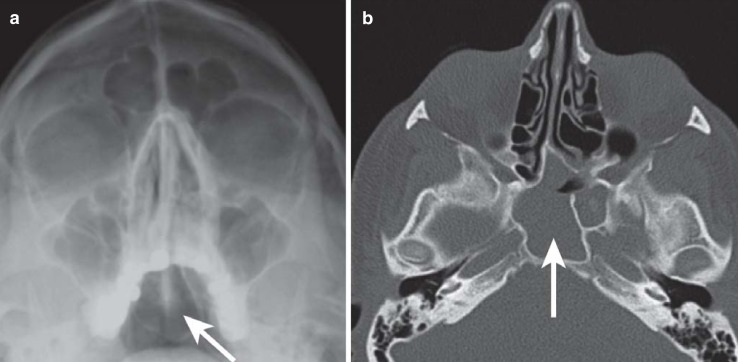
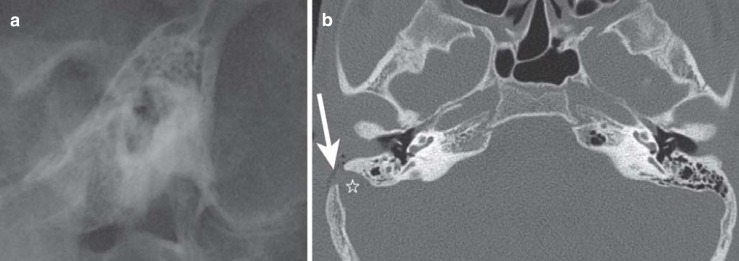
Background: Because of the complex anatomy of the head and neck region, conventional projection radiography alone is unreliable and carries a high risk of misdiagnosis. The poor risk-benefit ratio of conventional radiography has led to their replacement by tomographic imaging for nearly all studies in this region.
Method: This review is based on pertinent articles retrieved by a selective search in the PubMed database (January 1980 to May 2013) as well as on the relevant guidelines from Germany and abroad.
Results: The indication for diagnostic imaging in the anatomically complex head and neck region should be established for a specific type of imaging study on the basis of a thorough clinical examination. Conventional films, though easy to obtain, often cannot answer the diagnostic question and may yield confusing information leading to misdiagnosis. Computed tomography (CT) has the best risk-benefit profile and a high diagnostic value, but low-dose protocols have not yet been put into use in all centers. Magnetic resonance imaging (MRI) is best for bone and soft-tissue diagnosis, but consumes more resources. Digital volume tomography (DVT) is another type of three-dimensional, sectional imaging with high local resolution; the associated radiation exposure and image quality are generally both low, but may vary depending on the apparatus used. DVT cannot be used to evaluate the soft tissues. Ultrasonography can be used to evaluate superficial structures in the head and neck region; nuclear imaging can be used to evaluate thyroid disease and cancer.
Conclusion: Inflammatory, traumatic, and neoplastic diseases of the head and neck are best evaluated with cross-sectional imaging (CT, MRI) in accordance with current guidelines. Conventional x-rays should, in general, only be used for dental evaluation, with rare exceptions.
Figures
Comment in
-
Critical comments necessary.Dtsch Arztebl Int. 2015 Jan 30;112(5):69. doi: 10.3238/arztebl.2015.0069a. Dtsch Arztebl Int. 2015. PMID: 25686384 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2015 Jan 30;112(5):69. doi: 10.3238/arztebl.2015.0069b. Dtsch Arztebl Int. 2015. PMID: 25686385 Free PMC article. No abstract available.
References
-
- Sanders R, MacEwen CJ, McCulloch AS. The value of skull radiography in ophthalmology. Acta Radiol. 1994;35:429–433. - PubMed
-
- Mödder U. Nasennebenhöhlenerkrankungen - Möglichkeiten und Grenzen der Radiologie. Röntgenblätter. 1989;42:166–169. - PubMed
-
- Klimek L, Kainz J, Reul J, Mosges R. Vermeidung vaskulärer Komplikationen bei der endonasalen Nasennebenhöhlenchirurgie. Teil II: Prä- und intraoperative Bildgebung. HNO. 1993;41:582–586. - PubMed
-
- Mafee MF, Chow JM, Meyers R. Functional endoscopic sinus surgery: anatomy, CT screening, indications, and complications. AJR Am J Roentgenol. 1993;160:735–740. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical