

Patient perception of treatment burden is high in celiac disease compared with other common conditions
- PMID: 24980880
- PMCID: PMC4159418
- DOI: 10.1038/ajg.2014.29
Patient perception of treatment burden is high in celiac disease compared with other common conditions
Abstract
Objectives: The only treatment for celiac disease (CD) is life-long adherence to a gluten-free diet (GFD). Noncompliance is associated with signs and symptoms of CD, yet long-term adherence rates are poor. It is not known how the burden of the GFD compares with other medical treatments, and there are limited data on the socioeconomic factors influencing treatment adherence. In this study, we compared treatment burden and health state in CD compared with other chronic illnesses and evaluated the relationship between treatment burden and adherence.
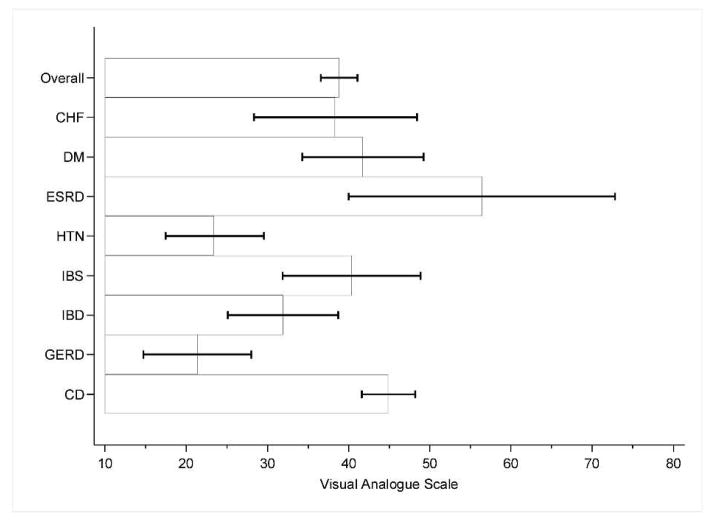
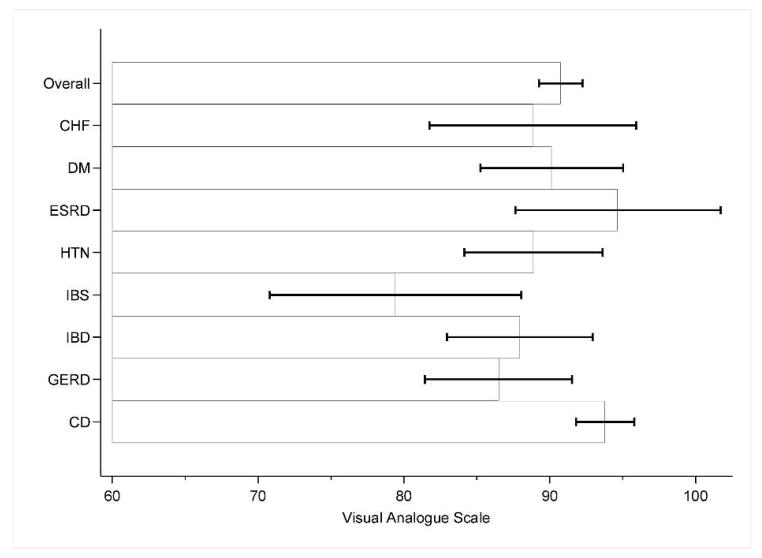
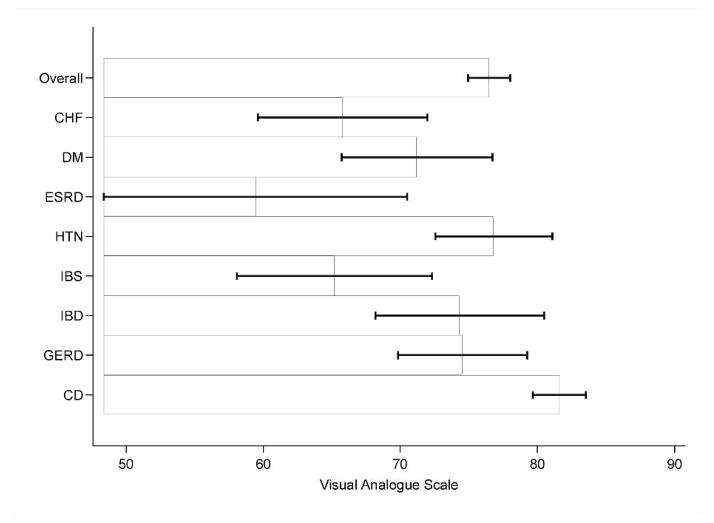
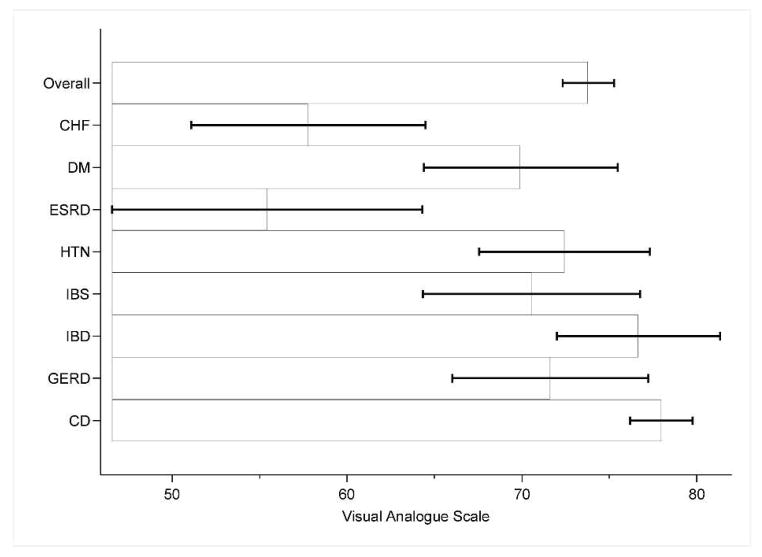
Methods: Survey was mailed to participants with CD, gastroesophageal reflux disease (GERD), irritable bowel syndrome, inflammatory bowel disease, hypertension (HTN), diabetes mellitus (DM), congestive heart failure, and end-stage renal disease (ESRD) on dialysis. Surveys included demographic information and visual analog scales measuring treatment burden, importance of treatment, disease-specific health status, and overall health status.
Results: We collected surveys from 341 celiac and 368 non-celiac participants. Celiac participants reported high treatment burden, greater than participants with GERD or HTN and comparable to ESRD. Conversely, patients with CD reported the highest health state of all groups. Factors associated with high treatment burden in CD included poor adherence, concern regarding food cost, eating outside the home, higher income, lack of college education, and time limitations in preparing food. Poor adherence in CD was associated with increased symptoms, income, and low perceived importance of treatment.
Conclusions: Participants with CD have high treatment burden but also excellent overall health status in comparison with other chronic medical conditions. The significant burden of dietary therapy for CD argues for the need for safe adjuvant treatment, as well as interventions designed to lower the perceived burden of the GFD.
Conflict of interest statement
Ciarán P. Kelly: None
Daniel Leffler: consulting and/or research support from: Shire Therapeutics, Prometheus Laboratories, Alba Pharmaceuticals, Alvine Therapeutics
Figures
References
-
- Lohi S, Mustalahti K, Kaukinen K, Laurila K, Collin P, Rissanen H, et al. Increasing prevalence of coeliac disease over time. Alimentary Pharmacology & Therapeutics. 2007;26(9):1217–25. - PubMed
-
- Fasano A, Berti I, Gerarduzzi T, Not T, Colletti RB, Drago S, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Archives of Internal Medicine. 2003;163(3):286–92. - PubMed
-
- Farrell RJ, Kelly CP. Celiac sprue. The New England journal of medicine. 2002;346(3):180–8. - PubMed
-
- Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA, Everhart JE. The prevalence of celiac disease in the United States. Am J Gastroenterol. 2012;107(10):1538–44. quiz 7, 45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
